| Pediculosis capitis = قمل الرأس |
|
|
PEDICULOSIS
Pediculosis Capitis (Head Lice)
EPIDEMIOLOGY
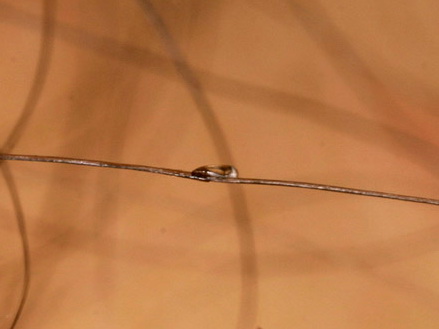
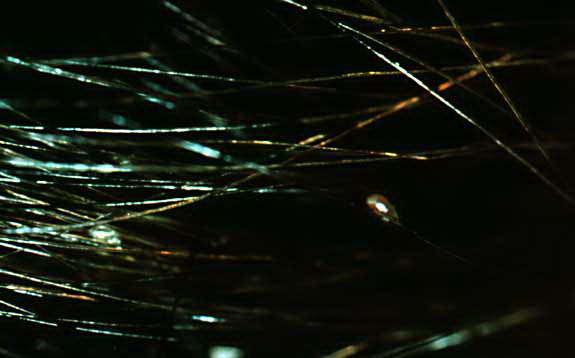
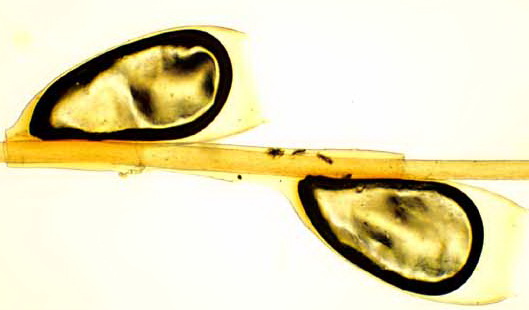
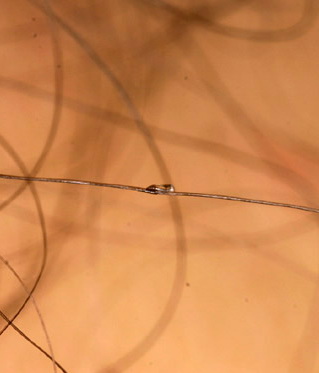
The head and body lice may be variants within a single species, but are thought by most biologists to represent two distinct species that can hybridize or interbreed under special circumstances. The most correct terminology at this time is Pediculus humanus var. humanus (body louse) and P. humanus var. capitis (head louse).31 Head lice infestations occur worldwide and are most common in school-aged children. Previous reports have estimated from 6 million to 12 million infestations occur each year in the United States among children 3 to 12 years of age, although this may be a gross underestimation given that many patients self-treat without reporting to health officials. The lice are spread by close physical contact as well as by the sharing of head gear, combs, brushes, and pillows. Head lice affect all levels of society and all ethnic groups, although in the United States, the incidence is low among African Americans. ETIOLOGY AND PATHOGENESIS The adult louse is 1 to 2 mm long, elongated, flattened dorsoventrally, and wingless. Head lice have three pairs of clawed legs that have been adapted to grasp hairs and can travel up to 23 cm per minute.31 The louse larva, called a nymph or instar, looks like a miniature adult louse. An adult louse must take a blood meal before copulation. A female louse can produce 5 to 10 eggs a day during her life span of 30 days. Lice typically survive only 1 to 2 days away from the scalp although under favorable conditions survival up to four days away from the scalp has been reported.31 Nits can survive for up to ten days away from the scalp.
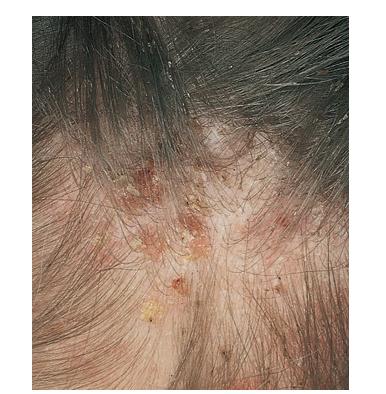
CLINICAL FINDINGS Pediculosis capitis is typically confined to the scalp with nits most often found in the occipital and retroauricular regions. Although patients can be asymptomatic, the most common symptom is itching and the sight of school children scratching their heads often leads to the diagnosis.
Differential Diagnosis of Head Lice Most Likely
Consider
Live nits are placed in close proximity to the scalp because the egg is reliant on warmth and moisture for incubation. Thus the distance of the nit from the scalp along the hair shaft is evidence of the duration of the infestation. When all of the nits are noted to be a significant distance from the scalp (i.e., more than 1 cm), it is likely that the infection is no longer active and that these nits are not fertile. Finding live adult lice, immature nymphs, and/or viable-appearing eggs confirms the diagnosis. Fine combing hair that has been saturated with water and conditioner appears to yield more positive results and fewer false positives than traditional scalp examination. Treatment for Head Lice
COMPLICATIONS Secondary bacterial infections may result, primarily due to excoriation. PROGNOSIS AND CLINICAL COURSE Untreated, head louse infestations may persist for many years. TREATMENT Pediculicides remain the most effective treatment for head lice. In general, pediculicides should not be used in children less than 2 years. To account for variable ovicidal activity and lack of full patient compliance, it is reasonable to recommend repeating treatment in 7 to 10 days to kill recently hatched nymphs. Wet combing involves combing systematically through wet, well-conditioned hair with a fine toothed comb every 3 to 4 days for a total of 2 weeks. Because lice are temporarily immobilized by water, wetting the hair allows easier removal by combing. Occlusive or suffocation methods, such as petroleum jelly or mayonnaise, have been used in the treatment of head lice for years. Although previous studies have failed to demonstrate an effective cure rate, newer agents [Cetaphil cleanser (initially labeled as Nuvo lotion)] have shown promise. In addition, new evidence indicates the nit sheath is composed of proteinaceous compounds instead of chitin-specific compounds, as was previously thought. With this knowledge attention has been turned toward agents that can effectively coat lice and eggs while either preventing formation or leading to degradation of the nit sheath. Oral agents offer the potential benefit of direct ingestion by the louse during blood meals. This in theory reduces the need for widespread application of chemical substances to promote absorption by the lice and therefore reduces risk of toxicity. Ivermectin has demonstrated systemic activity against head lice and should be considered as an alternative therapy . FAILURE AND RESISTANCE The only definite evidence of treatment failure is the presence of adult organisms. Treatment failure should be suspected if live lice are still present 12 to 24 hours after treatment. Possible contributors to treatment failure include changes in formulations, dilution of the pediculicide to an ineffective concentration when applied to wet hair, application of subtheraputic doses or duration in an attempt to conserve, or re-infestation from untreated contacts. Drug resistance has garnered much attention in recent years. Although treatment failure may contribute to resistance, examination of resistant populations has revealed the role of several different mechanisms. Mutations associated with knock down resistance are believed to affect highly conserved repeated domains in the sodium channel gene leading to permethrin-resistance. Other mechanisms
PREVENTION All members of the affected household should be examined. Although some physicians recommend treating all household members, others recommend treating affected individuals only. After therapy, the treated individuals should wear clean clothing, and both clothing and bedding should be washed and dried using the hot cycle; nonwashables should be dry cleaned, ironed, put in the clothes dryer without washing, or stored in a sealed plastic bag in a warm area for 2 weeks. Combs and brushes may be washed in very hot water (such as the dishwasher) and may be coated with the pediculicide first, for 10 or 15 minutes. Floors, play areas, and furniture should be carefully vacuumed to remove any hairs with viable eggs attached. Fumigation of living spaces is of no value. “No nit” policies requiring exclusion from school and treatment for all children with nits alone are likely excessive.
|
|||||||||||||||||||||||||||||||||