| Nevocytic Nevus = الوحمة وحمية الخلايا |
|
|
CONGENITAL
NEVOMELANOCYTIC NEVI
Epidemiology The vast majority of CNNs noted at birth are small and singular, and no gender predilection has been demonstrated. The most reliable prevalence rate for CNN in a homogeneous ethnic group was obtained by biopsying all pigmented lesions in 841 white infants examined within 72 hours of birth: Of 21 infants with pigmented lesions, 7 babies (0.83 percent of 841) had a biopsy-confirmed nevomelanocytic nevus. Many other series have yielded equivalent results. CNNs of 99 mm or more in diameter occur in only 1 of every 20,000
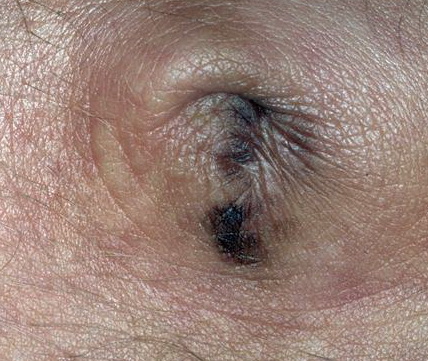
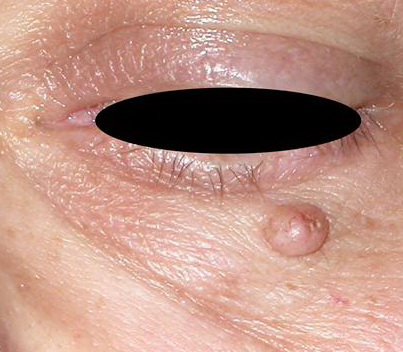
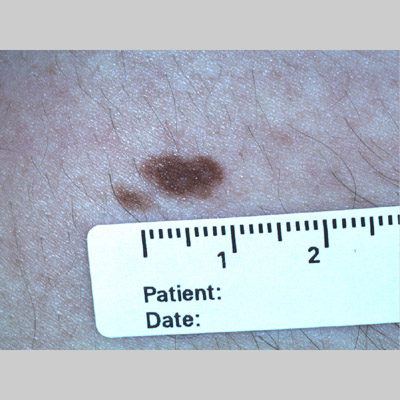
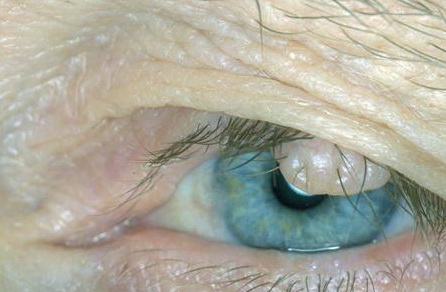
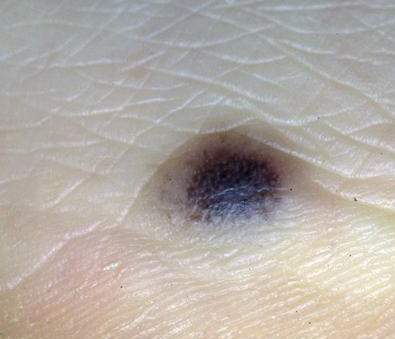
Etiology and Pathogenesis CNNs represent a developmental abnormality of normal melanocytic development. This is presumably due to mutation (potentially NRAS) that occurs in a progenitor cell that results in the abnormal extensive accumulation of melanocytic cells along migration pathways during normal development. The events leading to the nevomelanocyte accumulation may also have effects on the surrounding tissue (i.e., increased length/darker hair) possibly due to changes in the local cytokine environment of the nevomelanocytic cells. Clinical findings such as a congenital divided nevus of the eyelid can give us insight into when these events occur.8 The eyelids form at between 5 and 6 weeks in utero, begin to fuse at about 8 to 9 weeks, and reopen during the sixth uterine month.9 Because of the contiguous nature of this lesion on the upper and lower eyelids, it may be presumed that the nevomelanocytes migrated into this location sometime during or after eyelid fusion but before the eyelids split. HISTORY Most CNNs are present at birth; however, there are also rare varieties of relatively large nevomelanocytic nevi (> 1.5 cm) that appear for the first time between 1 month and 2 years of life, according to parental observations and corroborated by photographs (tardive congenital nevi). As a child grows, the CNN should grow relatively proportionally10 and continue to “mature.” History of disproportionate growth, especially after 6 months, or change in a non-uniform manner is of concern for possible melanoma. Both small and large varieties of CNNs have been associated with loss of pigmentation, halo depigmentation, and even regression. CUTANEOUS LESIONS Although CNNs are on average larger than acquired nevi, for lesions less than 1.5 cm in diameter there is no specific size limitation that can be used to predict reliably whether a given nevus is congenital or acquired. Lesions attaining a diameter of 1.5 cm or more are likely to be congenital, atypical melanocytic nevi, or melanoma. There is no completely satisfactory way to categorize CNNs as small or large. Definitions have been based on ease of removal and termed small if they can be excised and the wound defect closed primarily without significant deformity. Arbitrary size criteria have also considered small (< 1.5 cm; see eFig. 122-3.1 in on-line edition), medium (1.5 to 19.9 cm), and large (≥ 20 cm). Size, of course, is all relative to the location and the patient. Giant has been variously defined as a lesion as large as the patient's palm if it occurs on the head and neck (and twice that area for other anatomic sites), 30 percent of the body surface, or 900 cm2 in adults (or smaller if it involves a major anatomic area) (see Congenital Nevomelanocytic Nevus At a Glance figure). Depending on the definition used, lesions that are regarded as small or medium in the newborn period may be designated medium or large, respectively, by late childhood or adulthood, given that CNNs appear to grow in proportion to the affected anatomic site. The contour of CNNs is usually smooth, regular, and sharply demarcated, and skin markings distort the skin surface at least slightly when assessed by oblique lighting. Some CNNs are relatively hairless. However, coarse, long, darkly pigmented hair may be present at birth, appear within the first year or two of life, or be delayed for several years. Lesions may have a smooth, pebbly, rugose, verrucous, cerebriform, or grossly lobular surface. CNNs with a cerebriform appearance may present as cutis verticis gyrata. Dermoscopy may reveal a reticular pattern or globular/cobblestone pattern and may be useful in the identification of small foci of melanoma. In large congenital nevi, there can be significant variability in pigmentation and structure, and melanomas may develop in the deep components potentially reducing the utility of dermoscopy in these lesions. Unique varieties of CNNs may have an atypical appearance and be striking for their haphazard, very dark-brown, black, or blue-black pigmentation or discontinuous pigmentation and poorly demarcated and/or irregular outlines, often associated with atypical histopathologic features. Very darkly pigmented CNNs are distinctly uncommon in whites and should suggest the possibility of atypical histopathologic features. In darkly pigmented infants, CNNs are usually darkly pigmented. RELATED PHYSICAL FINDINGS CNNs of the head, neck, or posterior midline, and/or the presence of multiple satellite lesions associated with large CNN may be complicated by underlying cranial and/or spinal leptomeningeal melanocytosis. This phenomenon may be asymptomatic or may give rise to communicating or noncommunicating hydrocephalus, seizures, focal neurologic deficits, mental retardation, or even melanoma. CNNs need not be giant to be associated with this underlying disorder. There is a significant association between neurofibromatosis and giant CNNs. In a study by Crowe et al., 3 of 223 patients with neurofibromatosis had extensive CNNs. In his monograph on neurofibromatosis, von Recklinghausen described 1 of 28 patients as having a giant CNN.12 Tumors indistinguishable from neurofibroma in the absence of von Recklinghausen neurofibromatosis may develop in association with giant varieties of CNN. Malignant degeneration of large CNNs may be associated with the relatively sudden appearance of a dermal or subcutaneous nodule, very dark pigmentation, itching, pain, bleeding, or ulceration. Often, CNN-associated melanomas appear to have evolved in nonepidermal locations.13 Therefore, early detection of melanoma in association with a giant CNN may be difficult and not recognized until a dermal nodule or metastatic disease appears. The prognosis for patients who develop melanoma in association with giant CNNs is usually grave.13 Unlike melanoma in general, there is no ethnic predilection for melanoma developing in giant CNN. There have been multiple cases of lethal melanoma developing in association with giant CNNs in black children. Laboratory Tests HISTOPATHOLOGY CNNs are characterized by the presence of nevomelanocytes in the epidermis as well-ordered thèques and/or nevomelanocytes in the dermis which are present as sheets, nests, cords, and/or single cells. Although histopathologic features are cited as being useful in distinguishing nevi as congenital or acquired, there are no known features with absolute specificity and sensitivity. The histopathologic features of very large CNNs may be divided into nevomelanocytic, neuroid, epithelioid cell and/or spindle cell, blue, and mixed types. In the nevomelanocytic type of large CNN, the histopathologic appearance may be identical to typical acquired nevi, with nevomelanocytes in the epidermis as well-defined thèques and/or nevomelanocytes in the papillary dermis as sheets, cords, or nests. CNNs are more likely than acquired nevi to have nevomelanocytes in the lower two-thirds of the reticular dermis and to be associated with appendageal and neurovascular structures . There may be preferential involvement of one or more epithelial structures in CNN, such as eccrine ducts, and these structures may be abundant and malformed. Veins may be preferentially involved, with an “inflammatory” appearance showing nevomelanocytes within and around blood vessel walls. Subendothelial protrusion by nevomelanocytes in lymphatic vessels may be prominent. Arrector pili may be malformed, large, and infiltrated by nevomelanocytes. Hair follicles are often quite large and frequently associated with abundant melanin in the hair bulb. Nevomelanocytes in the deep reticular dermis may be distributed as single cells or as a single-file array insinuating among collagen bundles, sheets of cells, or combinations of patterns. Unique to the very large CNN is the occasional presence of nevomelanocytes within the substance of muscle, bone, placenta, umbilical cord, cranium, and dura mater. Very extensive CNN may be intermixed with elements of vascular malformation, hemangiomas, increased numbers of mast cells, cartilage, calcification, and even bone. There may be sparse mononuclear cell infiltrates associated with some giant CNNs. In addition to melanoma, associated tumors developing in CNN include schwannoma, neuroid tumor, lipoma, rhabdomyosarcoma, neurofibroma, sebaceous nevus, hemangioma, lymphangioma, and mastocytoma. A possible explanation for these mixed neoplasms containing melanocytic, neuronal, and other elements is that the CNN precursor cell, at least in some cases, is a pluripotent stem cell that has the capacity to give rise to multiple cell types. In giant CNNs, nevomelanocytes have been found in regional lymph nodes CNNs may also give rise to proliferative nodules that may be difficult to differentiate from melanoma. SPECIAL TESTS For patients with concern of possible leptomeningeal involvement, magnetic resonance imaging should be considered. For patients with concern of melanoma, positron emission tomography scan may be considered. Differential Diagnosis Complications The relationship between melanoma and large CNNs is well documented. The risk of melanoma development appears to be proportional to the size of the congenital nevus. The cumulative 5-year risk has been calculated to be 2.3 percent and 5.7 percent16 in patients with congenital nevi that involve over 5 percent of the body surface. The lifetime risk of melanoma for patients with very large CNNs has been estimated to be at least 6.3 percent, based on a questionnaire follow-up study of 151 persons with CNNs examined between 1915 and 1973 in Denmark. Melanoma may develop in large CNNs at any time, but the diagnosis of melanoma was established in the first 3 to 5 years of life in approximately one-half of published cases in which patients ultimately developed melanoma in association with giant CNN. A causal association between small CNNs and melanoma is more difficult to establish than for large CNNs. When histopathologic features were studied, 6 percent to 8 percent of primary melanomas were found to be in contiguity with nevi that had microscopic features characteristic of CNN.18,19 These findings support the concept of melanoma risk even with small congenital nevi, given the expected chance association based on body-surface-area considerations. Box 122-1 Differential Diagnosis of Congenital Nevomelanocytic Nevus
For cranial, midline, or CNN with multiple satellite lesions, there is a risk of leptomeningeal involvement. Symptomatic leptomeningeal melanocytosis carries a poor prognosis, even in the absence of malignant degeneration. Prognosis and Clinical Course CNNs have a dynamic evolution during body growth. CNNs at birth usually distort the skin surface at least slightly when assessed by oblique lighting and may become more elevated over time. Surface pigmentation also may change. Lightly pigmented CNNs may become more darkly pigmented, and darkly pigmented CNNs eventually may become less pigmented. CNNs also may develop a halo of depigmentation, potentially heralding spontaneous regression. Loss of pigmentation has been associated with regression of underlying nevomelanocytes and the replacement with sclerosis in some cases. Relatively hairless CNNs at birth may develop long, dark, coarse hair or may maintain a relatively normal hair density. With few exceptions, CNNs generally expand in direct proportion to growth of a given anatomic zone, although disproportionately rapid area expansion of some congenital nevi may occur during early infancy.10 Lesions in fully grown individuals should remain stable. Treatment The treatment of CNNs, large and small, depends on the perceived risk of melanoma plus cosmetic and functional considerations. Melanoma may arise in very large CNNs even in the first several years of life. Therefore, excision of very large CNNs should be considered as early as possible, but it is probably prudent to wait until after the first 6 months of life to reduce surgical and anesthetic risks. Management of patients with very large CNNs must be individualized. Extensive involvement of the body surface, with little or no normal skin available for graft sites, may necessitate abandoning efforts at prophylactic excision and accepting lifelong surveillance to detect the earliest signs of malignant change. It may be impossible to remove every nevomelanocyte in very large CNNs, particularly when there is involvement of vital structures or deep anatomic zones. The treatment goal is to remove as much of the nevus as possible while preserving function and improving cosmetic appearance. Tissue expansion and artificial skin replacement are invaluable in repairing large wound defects. Other indications for surgical excision of very large CNNs include chronic pruritus, ulceration, and infection. Unlike surgical excision, dermabrasion and other modes of destructive therapy do not address the malignant potential of CNN; nevomelanocytes may still be left behind in the dermis, and the cosmetic results associated with destructive therapy are unpredictable. Melanoma has been reported after dermabrasion of large CNNs.21 “Pseudomelanoma” has been described after laser treatment of a giant CNN.22 The approach to small CNNs needs to be considered carefully. It appears that the risk of melanoma development depends on CNN size, and therefore, smaller lesions appear to have less risk. However, due to the smaller size, complete excision of small congenital nevi may be relatively straightforward, resulting in excellent cosmetic results. Although atypical-appearing CNNs should be considered for immediate excision, careful surveillance without excision may be an option for clinically benign lesions depending on gross appearance, size, location, cosmetic and functional deficits (or improvement) resulting from excision, and general health issues. Given the risk of general anesthesia, for lesions perceived to be at low risk during the first decade of life it is appropriate to consider waiting until the child is old enough to tolerate local anesthesia. All CNNs should be documented at birth, preferably in the form of high-quality photographs that can be used to aid follow-up by parents and physicians. Follow-up is complicated by the natural evolutionary changes that take place in a nevus during body growth (i.e., surface, size, color, and hair), and periodic up-dates of photographs may be warranted. Suspicious changes in color, surface, or size require urgent evaluation. Prevention There is no known preventive approach to avoid the development of congenital nevi. Ultraviolet radiation (UVR)-induced mutations clearly play no role
|