| Norwegian scabies = الجرب النرويجي |
|
|
SCABIES
Epidemiology
Scabies is a human skin infestation caused by the penetration of the obligate human parasitic mite Sarcoptes scabiei var. hominis into the epidermis. The scabies mite is an arthropod of the order Acarina which was first identified in the 1600s, but was not recognized as the cause of the skin eruption until the 1700s. There are estimates that over 300 million people worldwide are infected with the scabies mite.2 Scabies affects all socioeconomic classes, with women and children being disproportionately infected. It tends to be more prevalent in urban areas, particularly in overcrowded regions. There is evidence of a seasonal variation, with more cases being diagnosed in the winter months than the summer. The incidence of scabies has been increasing over the past two decades, and has been found to be responsible for major outbreaks in nursing homes, prisons, and hospital wards. Transmission of the mite occurs usually through close personal contact, although the scabies mite can live off the human skin for up to 3 days, and therefore some infections can be from exposure to fomites.
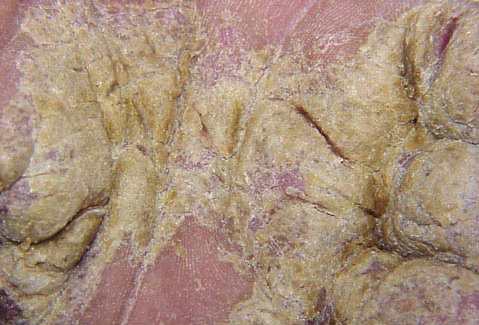
Etiology and Pathogenesis The scabies mite has four pairs of legs and measures 0.3 mm in diameter. It is therefore not easily seen with the naked eye. The mite cannot fly or jump; it lives its entire 30-day life cycle in and on the epidermis. The female mite burrows into the stratum corneum within 20 minutes and lays approximately 3 eggs a day. The eggs hatch after 4 days, and the larvae migrate to the skin surface and mature into adults.5 After 2 weeks, female and male mites copulate, after which the gravid female burrows back into the stratum corneum. The male, which is slightly smaller than the female, falls off the skin and perishes. The average number of mites a host harbors is usually less than 20, except in “crusted scabies” (previously known as Norwegian scabies), in which a host may harbor over a million mites.5 Individuals with human immunodeficiency virus, the elderly, and patients with medicationinduced immunosuppression are at risk of developing crusted scabies, although it has been reported among immunocompetent indigenous Australians.6 Clinical Findings After the initial exposure to the scabies mite, the pruritus and rash may take up to 6 to 8 weeks to develop. Subsequent exposure to the mite results in the itching and the rash developing within a couple days, probably due to prior sensitization to the scabies mite.7 The itching is severe and usually worst at night. The lesions appear as red, scaly, sometimes crusted (excoriated) papules and nodules that favor the interdigital webs , sides of the fingers, volar aspects of the wrists and lateral palms , elbows, axillae, scrotum,
In infants younger than the age of 2 years, the face and scalp can be infested, whereas in adults this is rarely the case. Erythematous to violaceous pruritic nodules found in the axillae and flanks of the trunk are not an unusual finding in children and on the scrotum in men , and are thought to be a hypersensitivity reaction to the mite. These nodules can remain for many weeks after the successful eradication of the mite infection. Vesicles and bullae may develop, particularly on the palms and fingers . In crusted scabies , hyperkeratotic plaques develop diffusely on the palmar and plantar regions, with thickening and dystrophy of the toenails and fingernails. The rest of the skin usually appears diffusely xerotic. Pruritus is variable and may be totally absent in this form of the disease. Over a million mites populate the skin and these highly contagious patients can be the source of outbreaks in health care facilities. The definitive diagnosis is made by the microscopic identification of the scabies mites, eggs, or fecal pellets (scybala). This is accomplished by placing a drop of mineral oil over a burrow and then scraping longitudinally with a number 15 scalpel blade along the length of the burrow, being careful not to cause bleeding. The scrapings are then applied to a glass slide and examined under low power (Fig. 208-5). Other diagnostic methods include dermoscopy (see Chap. 5) which can be used to examine the mite in vivo.10 A polymerase chain reaction-based method has been described in which the DNA from the mite was detected from cutaneous scales.11 A skin biopsy can be diagnostic, when the scabies mite is found transected in the stratum corneum . Differential Diagnosis Complications Secondary impetiginization is a common complication and usually responds well to either topical or oral antibiotics, depending upon the extent of the pyoderma. However, lymphangitis and septicemia can develop, particularly in crusted scabies . Post-streptococcal glomerulonephritis has resulted from scabies-induced pyodermas caused by Streptococcus pyogenes.12 Prognosis and Clinical Course If left untreated, the condition can persist for many years. In immunocompetent
Treatment There are a number of treatments for scabies which have various levels of effectiveness. Factors which may determine which treatment to use are the age of the patient, the cost of the medication, the severity of the eruption, and if previous treatments have been unsuccessful. In adults, topical scabicides should be applied to the entire skin surface, excepting the face and scalp, with special attention to the intertriginous areas, the genitalia, the periungual regions, and behind the ears. In children and those patients with crusted scabies, the face and scalp should also be treated. Patients must be informed that even after adequate scabicidal therapy, the rash and pruritus may persist for up to 4 weeks; otherwise they may believe that the prescribed treatment was unsuccessful, and then inappropriately overuse scabicidal medications. Topical steroids, antihistamines and, if necessary, a short course of systemic steroids, can be prescribed to alleviate the pruritus and rash once the patient has completed the scabicide treatment.. Treatment for Scabies
Differential Diagnosis of Scabies Most Likely
Consider
The only oral but highly effective scabicide known to date is ivermectin. It was discovered in the 1970s in the fermentation broth of a soil actinomycete Streptomyces avermitilis. It is structurally similar to macrolidic antibiotics, but with no antibacterial activity.16 It is currently U.S. Food and Drug Administration (FDA) approved for the treatment of the intestinal stage of onchocerciasis and strongyloides, but not FDA approved for the treatment of scabies. Its activity against the scabies mite is due to its high affinity for the gluminatedgated chloride ions found in the peripheral nervous systems of invertebrates.17 Ivermectin blocks the channel transmission across the nerve synapse that uses γ-aminobutyric acid. This results in the paralysis and death of invertebrate parasites. In mammals, these receptors are confined to the central nervous system and in normal conditions the drug does not cross the blood-brain barrier. It has been suggested that conditions that disrupt the blood-brain barrier may allow the drug to enter the central nervous system.18 Therefore the drug should not be used in children younger than the age of 5 years or weighing less than 15 kg, or during pregnancy or lactation, although there are reports of ivermectin being used in young children and during pregnancy without adverse effects.19 There are been numerous reports of the effectiveness of ivermectin in the treatment in scabies.20 The usual dosage is 200 µg/kg; often the dose is repeated in 10 to 14 days, but the optimal dosage schedule for the treatment of scabies has not been established. A clinical study comparing ivermectin to topical 5 percent permethrin revealed that a single dose of ivermectin provided a cure rate of 70 percent, which was increased to 95 percent with a second dose 2 weeks later. A single application of permethrin was curative in nearly 98 percent of patients.21 A topical preparation of 1 percent ivermectin has been shown to be effective in early clinical studies, but is not yet commercially available.22 In crusted scabies, the combination of ivermectin and a topical anti-scabicide is often used due to the severity of the infection, and multiple courses may need to be used to eliminate the infection. Side effects of ivermectin are usually mild and transient; however, there have been reported rare side effects of hypotension, laryngeal edema, and encephalopathy.23 There is one case report of an increased death rate in elderly nursing home patients who were treated with ivermectin.24 Subsequent studies have not confirmed this finding. Prevention Individuals in close contact with the infected person should be treated with a topical scabicide. Treatment should be directed to prevent spread of the scabies, because individuals may be harboring the scabies mite during the asymptomatic incubation period. Additionally, to prevent re-infection with fomites, bed sheets, pillow cases, towels, and clothes worn during the past 5 days should be washed and dried in the hot cycle, or be
|