













LYMPHEDEMA
Lymphedema is a consequence of prolonged edema; edema is an interference of the physiologic movement of fluid from capillaries through the interstitial spaces and back into lymphatics. In edema, the equilibrium is shifted and more fluid remains in the interstitial space—when this becomes chronic, inflammatory cells and their cytokines lead to an irreversible state.
Dysfunction of the lymphatic system because of genetic or congenital defects or related to infection, surgery, or external trauma leads to functional impairment of the tissue clearing ability and progression to clinical signs of lymphedema. The differential diagnosis of lymphedema is extensive but can be logically approached.
In all the clinical disorders discussed, edema may be transient and pitting with pressure but, with time, becomes fixed and accompanied by dermal sclerosis and epidermal hyperplasia.
Anatomy and Physiology of the Lymphatic System
Lymphedema-Related Genetic Diseases
Primary lymphedema (types I and II) is estimated at 1 in 6000. Other types are even rarer. A continuously updated
LYMPHEDEMA AT A GLANCE
· Lymphatics are essential for the clearing of extravascular fluids and debris and as transport of immunocompetent cells during the initiation of an immune response.
· Specific markers of lymphatic endothelia exist.
· Genetic defects causing lymphedema in childhood or early adult life are often caused by defects in a vascular growth factor receptor (VEGFR3) and FoxC2, a transcription factor.
· Lymphedema acquired in adult life is often related to chronic venous disease, after mastectomy with radiation and node removal, and, in certain geographic locations, filariasis.
· Cellulitis may complicate all forms of lymphedema and should be aggressively treated.
Etiology and Pathogenesis.
Type I lymphedema, an autosomal dominant disease characteristically has a mutation in VEGFR3 (also called the FLT4 gene). Penetrance is relatively high (80 percent). There is a 2.3:1.0 female predominance in pedigrees; this sex ratio may be due to a more severe disease in males that leads to hydrops fetalis and fetal death.
CLINICAL AND RADIOLOGIC FINDINGS
Lymphedema is almost always from birth and is confined to the legs with deep creases over the toes and small deformed (“ski jump”) toenails and is characterized hypoproteinemia from intestinal loss of albumen, chylous ascites, and scrotal edema.
Lymphangiography demonstrates dysplastic lymphatics in both clinically affected and clinically normal extremities, emphasizing the complexity of the pathophysiology, leading ultimately to disease. Prenatal ultrasound can show edematous legs in the fetus.
TYPE II LYMPHEDEMA (FORK-HEAD FAMILY
TRANSCRIPTION FACTOR DEFECTS)
Etiology and Pathogenesis.
The fork-head family transcription factor defects have in common mutations in a transcription factor, the fork-head transcription factor, FoxC2 [MFH1 (mesenchyme forkhead-1); fork-head is the name of a Drosophila trait]. FoxC2 is inherited as an autosomal dominant trait. The concept of type II lymphedema can be enlarged to include four syndromes with similar molecular defects: Lymphedema-late onset (Meige syndrome), lymphedema-distichiasis syndrome, lymphedema and ptosis syndrome, and the hereditary forms of lymphedema with the yellow nail syndrome. Mutations have included nonsense and frameshift mutations inactivating FoxC2.
Clinical Findings.
MEIGE SYNDROME
Edema develops around puberty, later than type I disease, and facial puffiness with deep creases and wrinkling may occur. Lymphedema praecox (Latin for premature) should not be used for this disease as it only leads to further nosologic confusion. Lymphangiosarcoma may be associated. Late on-set-type II disease has decreased or absent axillary nodes and decreased lymphatics above the inguinal ligament on scintilymphangiography.
Other rare syndromes with lymphedema exist.
GENETIC DISORDERS AFFECTING BOTH LYMPHATICS AND VEINS
ACQUIRED LYMPHEDEMA
Epidemiology.
Chronic edema in a community sample in London had a prevalence of 1.33 per 1000 and was 5.4 per 1000 for those older than the age of 65 years. Twenty-five percent of chronic edema was related to malignancy; and 29 percent of patients had at least one episode of cellulitis over the year before the survey; 70 percent to 80 percent of patients were female.
Worldwide lymphedema due to filariasis is estimated to affect between 90 and 100 million individuals . The microfilaria invade lymphatics, reproduce within the lymphatics, and damage local lymphatics and regional nodes, often resulting in hydroceles and scrotal swelling, classic components of filarial elephantiasis. In endemic areas, children may have subclinical disease that may be important to treat.
Other infectious diseases with lymphedema are much less common and include lymphogranuloma venereum with elephantiasis of the penis and scrotum, granuloma inguinale , and tuberculosis .
Etiology and Pathogenesis.
There are two major etiologies to non-hereditary lymphedema on a worldwide basis—venous disease of the legs (discussed earlier in this chapter) and postcancer, especially carcinoma of the breast-related lymphedema.
Clinical Findings.
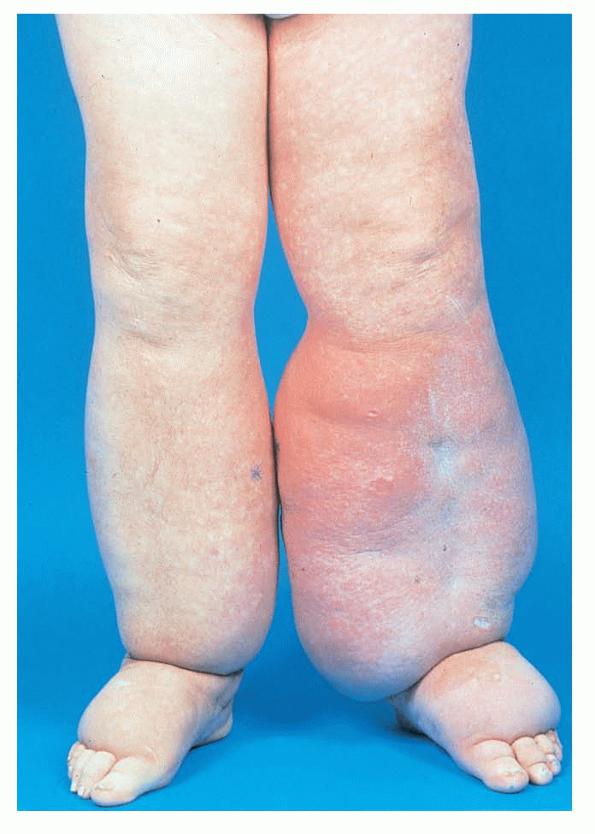
Acquired lymphedema is often painless and leaves legs feeling heavy and the patient tired. Although the limb swells during the day, indentations from socks can be seen on the leg at nighttime, returning toward normal during the night, but the leg stays swollen, and initially concerns may be cosmetic in nature. The foot is often involved first and initially lesions pit with pressure. With time, lesions become woody or lardaceous and do not pit. The toe contours are lost . Kaposi-Stemmer sign, a feature of chronic lymphedema, describes the skin over the proximal digit of the second toe that cannot be elevated; in edema the skin can be elevated.
Unilateral lymphedema suggests localized obstructing factors, but bilateral lymphedema can be due to obstruction in the pelvis or abdomen.
Inflammation with redness, pain, and swelling is not lymphedema but can be pyogenic infection, most commonly with S. aureus or Streptococcus pyogenes. Systemic antibiotics should be started before waiting for red lymphangitic streaking. A common complication is contact dermatitis from the use of topical antibiotics or multiple emollients and anti-inflammatory creams.
Special Tests.
Complications.
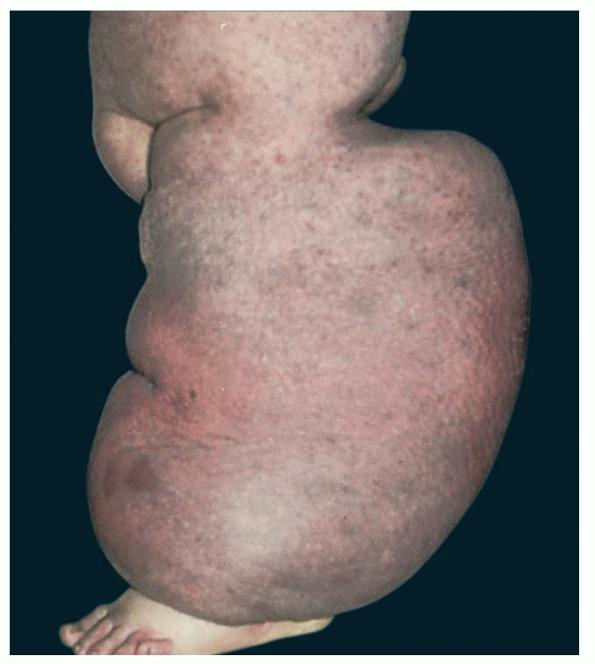
Prolonged lymphedema leads to fibrosis and epidermal hyperplasia with verrucous hyperkeratosis (Fig. 175-10). Ulceration rarely occurs, although the edema and hyperkeratotic changes may be profound. Lymphangiosarcoma, the Stewart-Treaves syndrome when associated with postmastectomy lymphedema, is the common lesion in chronically lymphedematous locations .
Prognosis and Clinical Course.
Careful, symmetric measurement at ankles, calves, and thighs should be made.
Treatment.
Diuretics may worsen the condition and should not be used as a primary treatment for lymphedema. Elevation,
massage, and sequential compression followed by elastic stockings can be used (see Treatment under Chronic Venous Disease). Various surgical approaches have been tried. In patients with primary and secondary lymphedema in the absence of venous or arterial disease, manual lymphatic drainage and sequential pneumatic pumps, in addition to compression wraps and garments, may be useful.
Cellulitis or recurrent lymphangitis is a significant problem in lymphedematous sites, and there is both a rationale and results that encourage long-term antibiotic use (e.g., 2.4 million units of benzathine-penicillin G intramuscularly every 2 weeks).
Microsurgery of lymphatics to bypass obstructed nodes can be considered if nonsurgical treatments are not successful. This surgery consists of the formation of multiple end-to-end lymphaticvenous anastomoses.
Excisional or suction-assisted lipectomy (liposuction) may be an option in selected patients.
Prevention.
Any patient with lymphedema, whatever the cause, should keep their feet dry, nails trimmed, and prevent and aggressively treat pyogenic infection. Lymph moves faster during limb activity and exercise (e.g., walking should be encouraged).
LOCALIZED AREAS OF LYMPHEDEMA
Lymphedema is common in some locations, face and penis especially; low-grade infection is usually invoked as the cause.
In puffy hand syndrome, intravenous drug use with injections into hands or feet is associated with lymphedema. The condition is not drug specific.