| Livedo Reticularis =الترخم الشبكي |
|
|
LIVEDO RETICULARIS -AND
LIVEDO RACEMOSA
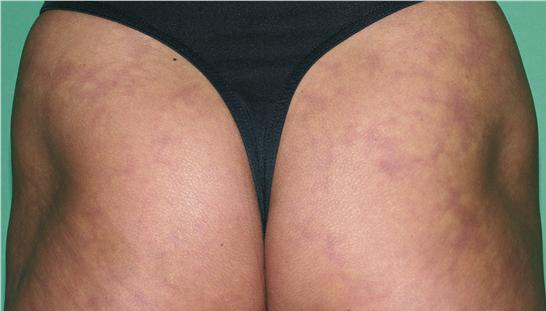
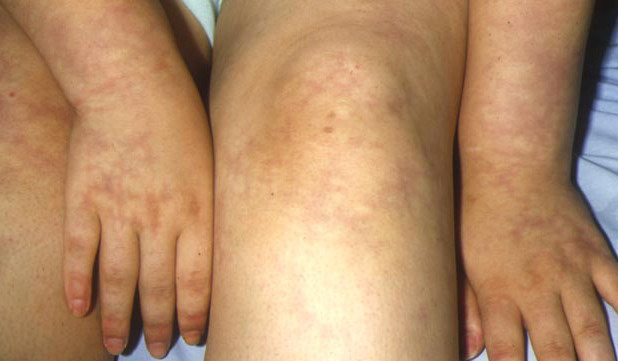
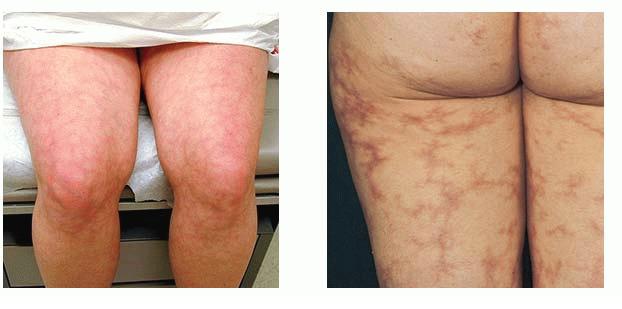
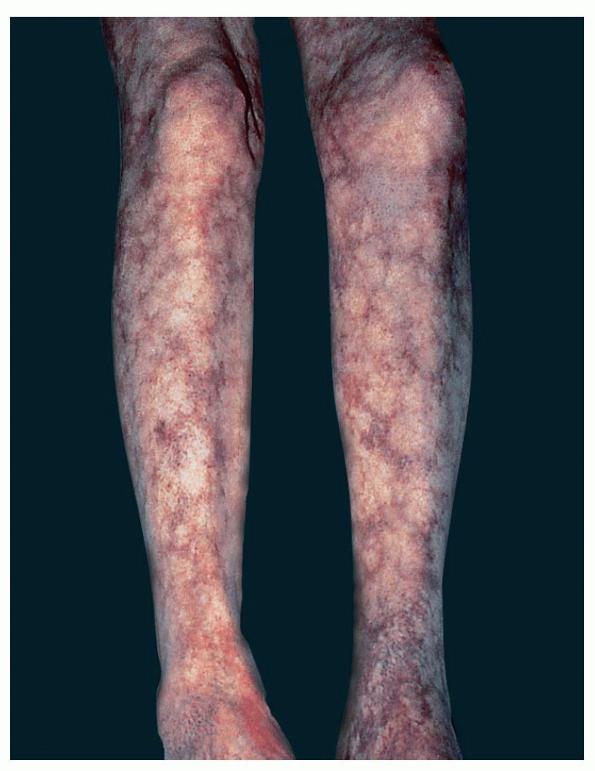
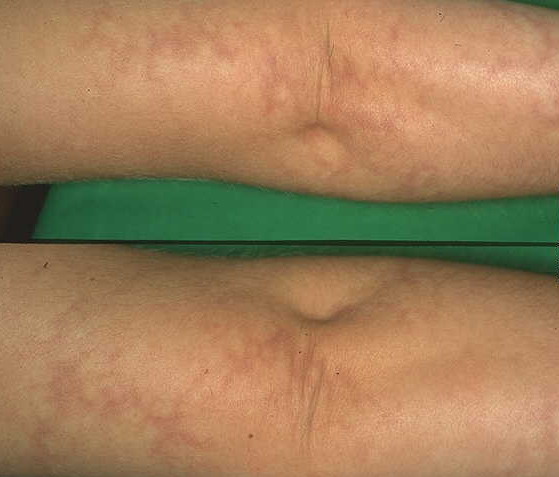
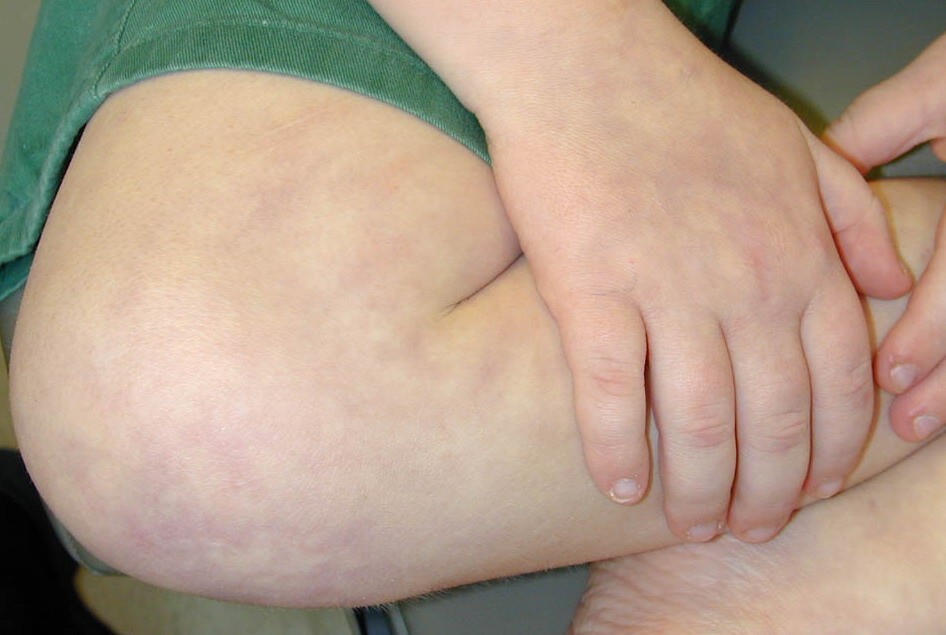
Epidemiology Livedo reticularis is typically a primary disorder that affects young to middle-aged females (20 to 50 years of age) who are otherwise healthy. Amantadine-induced livedo reticularis is also more common in females. The epidemiologic factors of livedo racemosa are dependent on the underlying condition. The distinction between livedo racemosa and livedo reticularis is an evolving concept, which is not universally quoted, and is not referenced in most of the older literature. Etiology and Pathogenesis In both disorders, the characteristic ringlike mottling results from (patho)physiologic changes with the cutaneous microvascular system. Anatomically, the dermis is perfused via perpendicularly oriented ascending arterioles. Individual arterioles arborize into a capillary bed at the skin surface. Ultimately, the capillary beds empty into a conical appearing, peripherally located subpapillary venous plexus. Pathophysiologically, livedo arises from either deoxygenation or venodilatation within the venous plexus. Decreased arteriolar perfusion is the predominant cause of deoxygenation within the venous plexus. Diminished arteriolar flow can result from vasospasm, hyperviscosity, and/or thrombosis. Physiologic arteriolar vasospasm produces the reversible cutaneous discoloration of livedo reticularis. Protracted arteriolar vasospasm, thrombosis and/or hyperviscosity underlie the pathologic skin changes of livedo racemosa. Venodilatation of the venous plexus may be provoked by hypoxia or autonomic dysfunction. Amantadine-induced livedo reticularis has traditionally been ascribed to catecholamine provoked arteriolar vasospasm; however, an interaction between amantadine and N-methyl-D-aspartic acid receptors in the skin may be responsible in some unexplained fashion. Livedoid vasculopathy is a rare ulcerative sub-type of livedo racemosa due to fibrinolytic abnormalities and microcirculatory thrombosis. Clinical Findings HISTORY With the exception of a subjective feeling of coldness, the majority of patients with livedo reticularis are asymptomatic. Patients often present with concerns regarding their skin discoloration. A minority describe mild pain and numbness. Livedo racemosa-associated symptoms are related to the causative secondary disorder (e.g., livedoid vasculopathy provokes painful ulcerations). CUTANEOUS LESIONS In livedo reticularis, a symmetric, fishnet-like red or purple mottling surrounds a pallorous conical core . This discoloration is aggravated by cold exposure and may completely dissipate with warming. The livid rings are most pronounced on the lower extremities yet the abdomen and upper extremities can be affected. In contradistinction to the symmetric and uniform reticular pattern of livedo reticularis, the discoloration of livedo racemosa is asymmetric, irregular, and “broken” . Although it may improve with warming, it does not resolve. Attendant skin manifestations of livedo racemosa may include purpura, nodules, macules, ulcerations, and/or atrophie blanche type scarring. In both livedo reticularis and racemosa, the skin is palpably cool. RELATED PHYSICAL FINDINGS Livedo reticularis and livedo racemosa are often associated with vasospastic digits or acrocyanosis. With exception of the characteristic skin changes, the examination in livedo reticularis is otherwise unremarkable. Patients with livedo racemosa may have concurrent abnormal physical findings related to their underlying disease (e.g., aphasia and lateralizing neurologic signs associated with Sneddon syndrome). Laboratory and Special Tests In livedo reticularis, laboratory testing is typically negative and consequently is unwarranted. A skin biopsy is not required in livedo reticularis as the findings are non-specific. A large punch or wedge biopsy of the deep reticular dermis and subcutaneous fat is sometimes helpful in identifying the secondary cause of livedo racemosa. The biopsy findings are highly variable and reflect the associated livedo racemosa etiology. For instance, cholesterol clefts suggest atheroembolic disease, calcification of the vessels and interstitium indicate calciphylaxis, noninflammatory arteriolar obstruction occurs with Sneddon syndrome, livedoid vasculopathy is associated with extensive fibrin deposition and microthrombi , whereas fibrinoid necrosis is present in polyarteritis nodosa . Differential Diagnosis The diagnosis of livedo is easily made by identifying the characteristic mottled skin discoloration. It is paramount that the clinician distinguish between livedo reticularis and livedo racemosa. Once a diagnosis of livedo racemosa is established, the secondary cause should be sought . Prognosis and Clinical Course The prognosis for livedo reticularis is excellent as this is primarily a cosmetic condition. Livedo racemosa-associated prognosis is less favorable and parallels the associated disease. Of interest, livedo racemosa has been identified as a marker for predicting multisystem thrombosis in the anti-phospholipid antibody syndrome. Additionally, up to 40 percent of patients manifest livedo racemosa as the initial sign of the anti-phospholipid antibody syndrome.7 Livedoid vasculopathy tends to be a relapsing condition marked by recurrent painful ulcerations and subsequent atrophie blanche type scars. Treatment Other than cold avoidance, medical treatment for primary livedo reticularis is typically unwarranted. As a last resort, vasodilator therapy may be tried in the patient that is socially inhibited by the cosmetic appearance of the disorder.
Therapy of livedo racemosa should be directed towards the underlying disorder. Patients with livedo racemosa and the anti-phospholipid antibody syndrome with thrombosis require anticoagulation. Treatment of livedoid vasculopathy is often unsatisfactory but potentially beneficial medications include anticoagulants, anti-platelet agents, immunosuppressants, pentoxifylline, danazol, and tissue plasminogen activator. Alternatively, hyperbaric oxygen and psoralen and ultraviolet A light therapy have also been successfully utilized to treat livedoid vasculopathy.
|