LEUKEMIA CUTIS
Leukemia cutis (LC) is a localized or disseminated skin infiltration by leukemic cells. It is usually a sign of dissemination of systemic disease or relapse of existing leukemia. Reported incidence varies from less than 5 percent to 40 percent, depending on the type of leukemia, both acute and chronic, including the leukemic phase of non-Hodgkin lymphoma and hairy cell leukemias. It most commonly occurs with acute monocytic leukemia, M5, and acute myelomonocytic leukemia, M4.
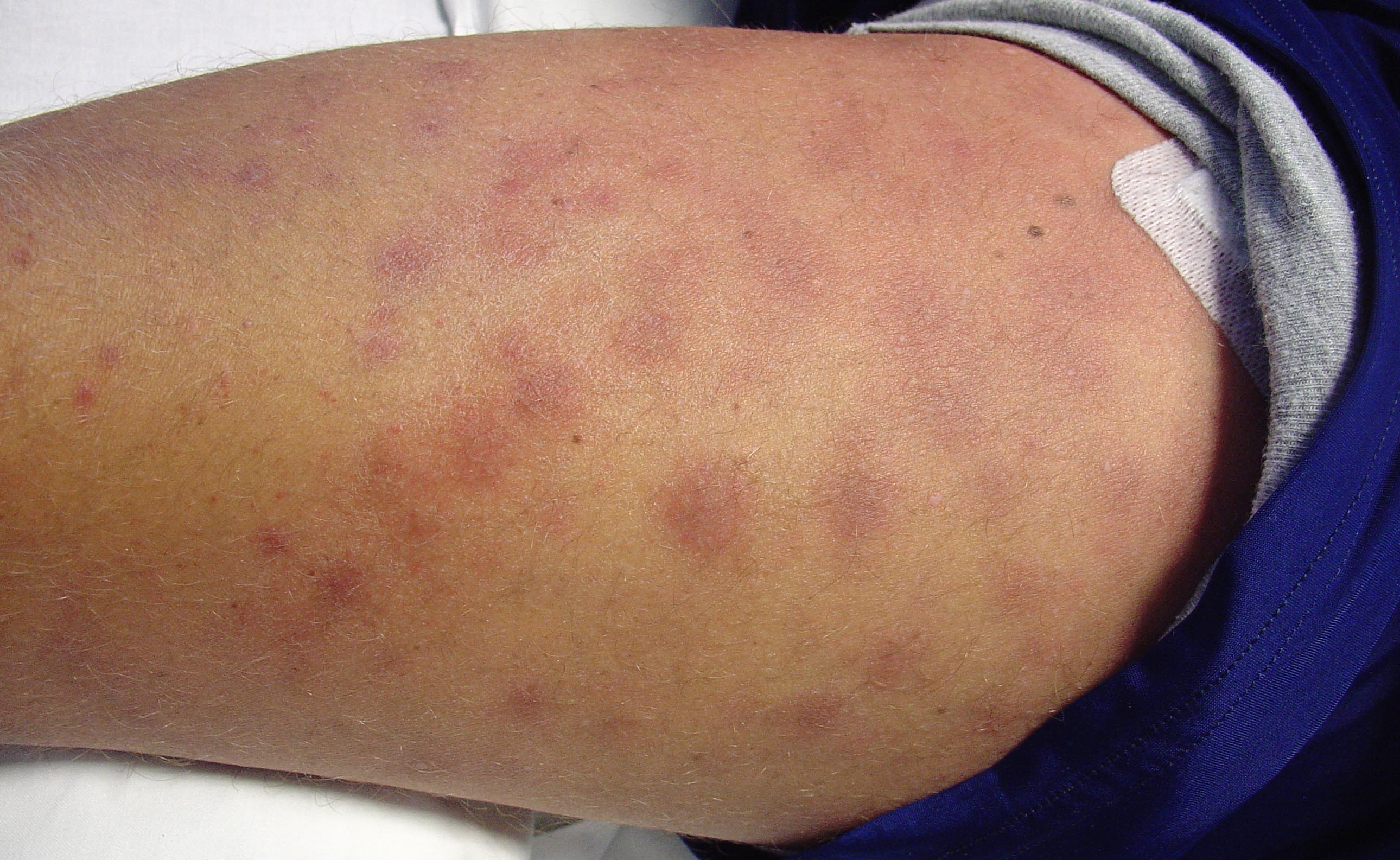
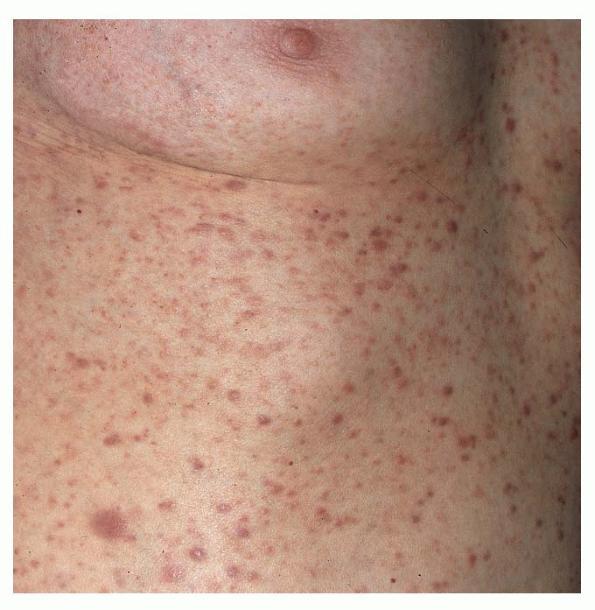
Pattern of presentation of skin lesions in LC is variable and may have features that overlap with other (inflammatory) eruptions. Most common lesions are small (2 to 5 mm) papules , nodules , or plaques. LC lesions are usually somewhat more pink, violaceous, or darker than normal skin, always palpable, indurated, firm, or guttate psoriasiform or lymphomatoid papulosis-like lesions, but usually not tender. They are localized or disseminated; usually on trunk , extremities, and face) but may occur at any site. They may be hemorrhagic when associated with thrombocytopenia or may ulcerate
. Erythroderma may (rarely) occur. Leukemic gingival infiltration (hypertrophy) occurs with acute monocytic leukemia. Similar lesion morphologies occur with different types of leukemia or specific types of leukemia may present with a variety of morphologies
.
|
Clinical Conditions Associated with Disseminated Intravascular Coagulation
|
|
· Sepsis/severe infection (any microorganism)
· Trauma (e.g., polytrauma, neurotrauma, fat embolism)
· Organ destruction (e.g., severe pancreatitis)
· Malignancy
o Solid tumors
o Myeloproliferative/lymphoproliferative malignancies
· Obstetric calamities
o Amniotic fluid embolism
o Abruptio placentae
· Vascular abnormalities
o Kasabach-Merritt syndrome
o Large vascular aneurysms
· Severe hepatic failure
· Severe toxic or immunologic reactions
o Snake bites
o Recreational drugs
o Transfusion reactions
o Transplant rejection
|
|
Inflammatory disorders occurring in patients with leukemia are modified by the participation of leukemic cells in the infiltrate, resulting in unusual presentations of such disorders (e.g., psoriasis with hemorrhage or erosions/ulcerations). Also, there are a number of cutaneous inflammatory diseases that may be associated with leukemia: Sweet syndrome (, bullous pyoderma gangrenosum , urticaria , and necrotizing vasculitis .
Systemic symptoms are those associated with hematologic malignancy. Not infrequently, cutaneous manifestation may be the initial presenting symptom and may contribute importantly to the diagnosis.
The diagnosis is made by suspicion and verified by skin biopsy, immunophenotyping, and B- or T-cell receptor rearrangement studies. Hematologic studies with complete analysis of bone marrow aspirate and peripheral blood smear are then needed to make the diagnosis. If cutaneous findings precede any systemic disease, careful assessment of peripheral blood smears and bone marrow biopsies must be made.
The prognosis of LC is directly related to the prognosis for systemic disease. Therapy is usually directed at the leukemia itself.