|
Angioedema= الوذمة الوعائية |
 |
 |
 |
Angioedema
Angioedema is the swelling of deep dermis, subcutaneous or submucosal tissue due to vascular leakage.1 It was first described in 1586.2 Other terms, such as giant urticaria,3 Quincke edema,4 and angioneurotic edema,5 have also been used in the past to describe this condition. Clinically, angioedema is usually nonpitting and nonpruritic. The area of involvement is often skin-colored or slightly erythematous. Depending on the area of swelling, pain can be absent or mild, as in most peripheral or facial swelling, or can be very severe, as in gastrointestinal angioedema. Laryngeal swelling is life-threatening. It should be treated as a medical emergency.
Angioedema is often associated with urticaria. In fact, almost 50% of patients who present with urticaria also have angioedema.6 Angioedema, with or without concurrent urticaria, may often have different etiologies. This article concentrates on angioedema without urticaria. For angioedema associated with urticaria, the treatment strategies are essentially the same as discussed in eMedicine article Urticaria. Hereditary angioedema (HAE) and acquired angioedema (AAE), special types of angioedema caused by decreased functional C1-esterase inhibitor (C1-INH), are discussed in eMedicine article Hereditary Angioedema.
Pathophysiology
The swelling of the affected area of angioedema is a result of the fast onset of increase of local vascular permeability in submucosal and subcutaneous tissue. IgE-mediated mast cell activation and degranulation, key elements of an allergic reaction, often manifest as urticaria and angioedema. Non–IgE-mediated mast cell activation/mediator release may explain certain autoimmune-mediated and idiopathic angioedema.7 In addition to mast cells, many other cells, such as macrophages, dendritic cells, lymphocytes, monocytes, eosinophils, and endothelial cells, have been shown to be involved in the pathogenesis of angioedema.1,8 Plasma and tissue factors, such as bradykinin, and certain components in contact system or fibrinolytic systems are also found to play an important role in certain forms of angioedema.9,10
Urticaria is often discussed together with angioedema. In many cases, they are remarkably similar, both in underlying etiologies and clinical management strategies. On the other hand, angioedema is also quite different from urticaria. It usually involves a deeper layer of skin (reticular dermis) or subcutaneous or submucosal tissue, whereas urticaria affects a more superficial layer of skin (papillary dermis and mid dermis). In fact, mucosal involvement is observed in angioedema but not in urticaria. In addition, pruritus is the most prominent complaint in urticaria but is less troublesome or absent in angioedema. Furthermore, pain or tenderness is uncommon in urticaria but frequent or even severe in angioedema. Addressing these differences is necessary for successful treatment of angioedema
Angioedema is one of the most troubling complications of an acute allergic reaction. In one study, 69.4% of 138 patients who had anaphylaxis were found to have angioedema.16 In addition to the disfiguring appearance, patients often report local pain and discomfort. When angioedema affects the hands and feet, walking and many other daily activities are impaired. Abdominal pain is common when the gastrointestinal tract is involved; it can be severe and disabling
Patients usually describe swelling of the face (eg, eyelids, lips), tongue, hands, and feet. It can be acute or chronic, and each episode of angioedema may last a few hours to a few days. A local burning sensation and pain can be observed without pronounced itchiness or local erythema. Abdominal pain can sometimes be the only presenting symptom of angioedema. Throat tightness, voice changes, and trouble breathing may indicate airway involvement.
For acute and new-onset angioedema, special attention should be directed to the potential relationship with food or drug intake, insect stings, or other unusual exposures. For chronic and recurrent cases, ask the patient about potential triggers, medication use and associated medical history, family history, and past evaluation.
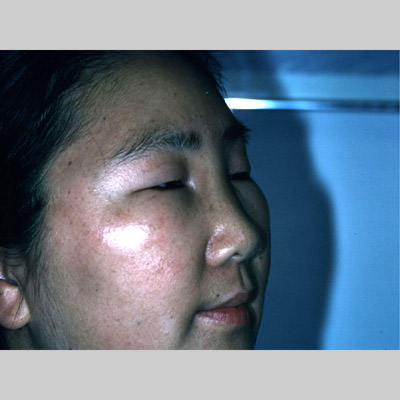
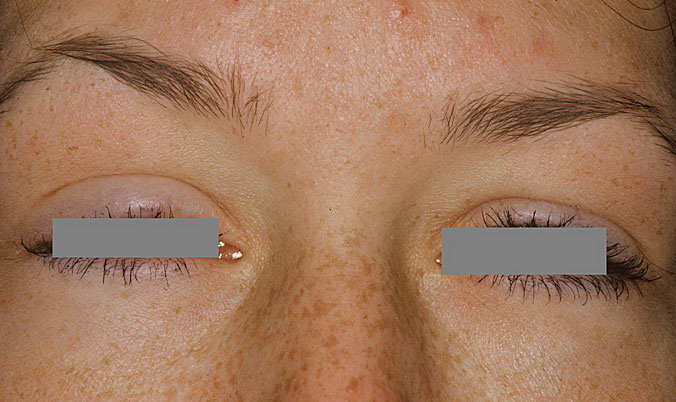
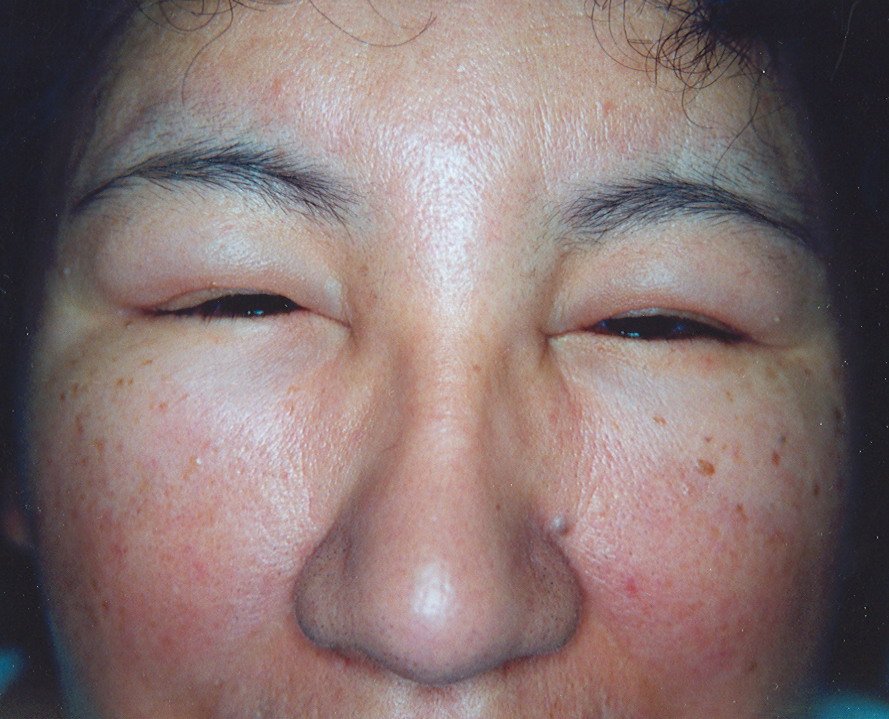
Physical
For skin involvement, examination can easily identify areas of swelling with or without erythematous skin, often with ill-defined margins. Some cases of angioedema occur in patients with urticaria.
The examination of abdominal (intestinal mucosal) angioedema can be challenging. The patient may have changes in bowel sounds and diffuse or localized tenderness. Some cases may resemble an acute abdomen.
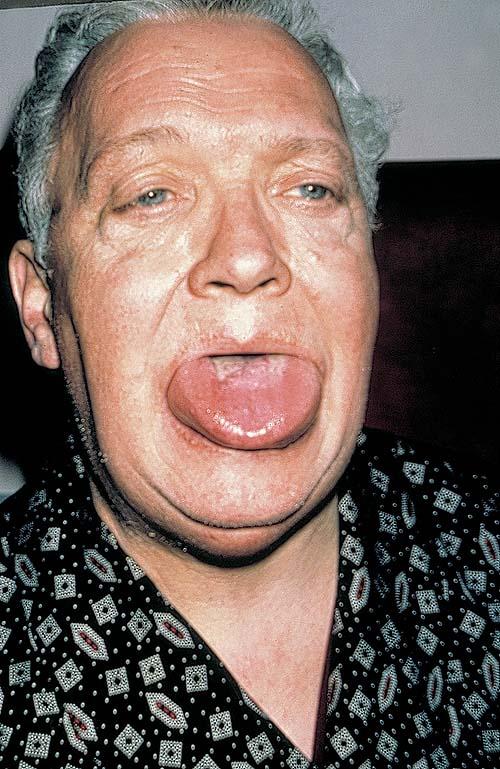
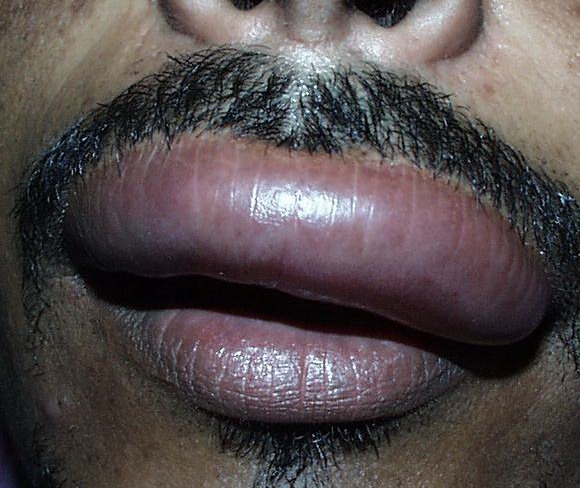
Uvula or tongue swelling can be visualized directly (see image below). However, a laryngoscopy is needed to assess laryngeal or vocal cord involvement.
Angioedema can be life-threatening when it involves the larynx and upper airway, leading to trouble breathing, asphyxia, and even death. Of angioedema presented in the emergency room, 10-25% of cases are considered to be life-threatening
Causes
Angioedema can be categorized as allergic, pseudoallergic, nonallergic, or idiopathic. More than 40% of chronic angioedema is idiopathic. All cases of angioedema pose significant diagnostic and treatment challenges.
Allergic angioedema
- Allergic angioedema is often associated with urticaria. It is typically observed within 30 minutes to 2 hours after exposure to the allergen (eg, food, drug, venom, latex). Brown et al reported 142 patients with anaphylaxis who presented in the emergency department. Angioedema was present in 40% of the cases (49.3% of those with urticaria).19
- More detailed description of this condition can be found in the eMedicine articles Anaphylaxis and Urticaria.
Pseudoallergic angioedema
- Pseudoallergic angioedema is not IgE-mediated. However, its clinical course and presentation is very similar to allergic angioedema. Typical examples are angioedema induced by nonsteroidal anti-inflammatory drugs (NSAIDs) and intravenous contrast material; aspirin (ASA) is the most common culprit.
- True IgE-mediated reactions to ASA or other NSAIDs are uncommon. The angioedema (with or without urticaria) reflects the pharmacologic properties of the drugs. By inhibiting cyclooxygenase (COX), ASA and NSAIDs lead to overproduction of proinflammatory and vasoactive leukotrienes. COX-2 inhibitors and acetaminophen do not usually cause angioedema.
Nonallergic angioedema
- Nonallergic angioedema does not involve IgE or histamine; urticaria is generally not associated with this type of angioedema.
- Hereditary angioedema (HAE) is perhaps the prototype of this type of angioedema. Decreased functional C1-INH production leading to unchecked bradykinin production are believed to be the fundamental changes in HAE types I and II.20 Acquired angioedema (AAE) also has decreased C1-INH function due to autoantibody production or accelerated consumption of C1-INH. Please see the eMedicine article on HAE for additional details on these conditions.
- ACE inhibitor–induced angioedema (AIIA) is bradykinin-mediated, as in cases of HAE and AAE. Most AIIA is observed in the first week after starting the medicine; however, up to 30% of AIIA starts months or even years after starting the medicine.15,21 Therefore, it can easily be overlooked as a cause for angioedema. AIIA is not drug-specific. As illustrated in the image below, ACE inhibitors interfere with the degradation of bradykinin, a potent vasoactive nonapeptide.
Idiopathic angioedema
- The causes of idiopathic angioedema are, by definition, not identifiable. Furthermore, the exact mechanisms are unclear.11,12 Some may be associated with urticaria. Based on responses to medication, some cases are thought to be mediated by mast cell activation, albeit IgE-independent.
- Physical urticaria/angioedema: Common triggers include heat, cold, emotional stress, and exercise. Nonspecific mast cell activation and degranulation are suspected causes.
- Autoimmune conditions: Thyroid autoantibodies are found in 14-28% of patients with chronic urticaria/angioedema, and IgG autoantibodies to either the high affinity receptor for IgE (FceRI) or to IgE are found in 30-50% of patients with chronic urticaria/angioedema.11,22 In affected individuals, autoantibody (IgG) has been found to crosslink FceRI on mast cells, resulting in mast cell activation and release of histamine, cytokines, and other proinflammatory mediators. Immunomodulatory drugs may be beneficial for this type of angioedema.23
- Infections: The link between infection and angioedema is vague at best. Helicobacter pylori infection has been found to be associated with HAE exacerbation. Treatment of H pylori infection has led to clinical improvement of chronic urticaria and angioedema.24 Systemic viral, bacterial, or parasitic infection may stimulate the immune system and cause improper activation or inflammatory changes.
- Estrogen-dependent angioedema: C1-INH functions normally in estrogen-dependent angioedema.25 This has been proposed as HAE type III. The exact mechanism of angioedema in these patients is still unclear.18 In some of the affected patients, FXII point mutation results in a gain of function that can potentially affect the metabolism of bradykinin.26
- Gleich syndrome: Patients with this syndrome exhibit elevated eosinophil with angioedema. It responds well to corticosteroids. It is thought to be related to hypereosinophilic syndrome.27 In addition to the elevated eosinophils count, IgG autoantibody against endothelial cells has been identified.
|
|
|
|