Androgenetic alopecia
Androgenetic alopecia, or pattern alopecia, is an extremely common disorder affecting both men and women. The incidence of androgenetic alopecia is generally considered to be greater in males than females, although some evidence suggests that the apparent differences in incidence may be a reflection of different expression in males and females.
Pathophysiology
Androgenetic alopecia is a genetically determined disorder and is progressive through the gradual conversion of terminal hairs into indeterminate hairs and finally to vellus hairs. Patients with androgenetic alopecia have a reduction in the terminal-to-vellus hair ratio, normally about 4:1. Following miniaturization of the follicles, fibrous tracts remain. Patients with this disorder usually have a typical patterned distribution of hair loss.
In androgenetic alopecia, Studies have indicated a self-renewal of the hair follicle via keratinocyte stem cells located at the area of the bulge of the hair follicle. In addition, a series of studies using mice has indicated that interfollicular keratinocyte stem cells could generate de novo hair follicles in adult mouse skin. These regenerated hair follicles cycled through stages of telogen to anagen. However, these transitions between bulge and epidermal keratinocytes have not been seen yet in human studies.1
Another report has indicated that mice lacking in functional vitamin D receptors develop a functional first coat of hair, but lack the cyclic regeneration of hair follicles leading to the development of alopecia.2 Whether these findings will lead to a new area of exploration into the cause of androgenetic alopecia in humans is unknown at this time.
Frequency
International
Androgenetic alopecia is an extremely common disorder that affects roughly 50% of men and perhaps as many women older than 40 years. As many as 13% of premenopausal women reportedly have some evidence of androgenetic alopecia. However, the incidence of androgenetic alopecia increases greatly in women following menopause, and, according to one author, it may affect 75% of women older than 65 years.
A community-based study of androgenetic alopecia in 6 cities in China indicated that the prevalence of androgenetic alopecia in both Chinese males and females was lower than that seen in whites but similar to the incidence among Koreans
History
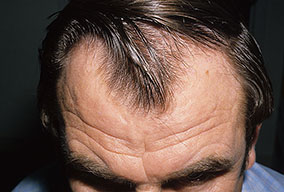
The onset of androgenetic alopecia is gradual. Men present with gradual thinning in the temporal areas, producing a reshaping of the anterior part of the hairline. For the most part, the evolution of baldness progresses according to the Norwood/Hamilton classification of frontal and vertex thinning. Women with androgenetic alopecia usually present with diffuse thinning on the crown. Bitemporal recession does occur in women but usually to a lesser degree than in men. In general, women maintain a frontal hairline.7
Physical
In both males and females with androgenetic alopecia, the transition from large, thick, pigmented terminal hairs to thinner, shorter, indeterminate hairs and finally to short, wispy, nonpigmented vellus hairs in the involved areas is gradual. As the androgenetic alopecia progresses, the anagen phase shortens with the telogen phase remaining constant. As a result, more hairs are in the telogen phase, and the patient may notice an increase in hair shedding. The end result can be an area of total denudation. This area varies from patient to patient and is usually most marked at the vertex.
Women with androgenetic alopecia generally lose hair diffusely over the crown. This produces a gradual thinning of the hair rather than an area of marked baldness. The part is widest anteriorly. The frontal hairline is often preserved in women with this disorder, whereas men note a gradual recession of the frontal hairline early in the process.
Causes
Androgenetic alopecia is a genetically determined condition. In 2008, 95 families were studied genetically, and the locus with strongest evidence for linkage to androgenetic alopecia was the 3q26 site on the X chromosome.8 In addition, an association between androgenetic alopecia and chromosome 20pll and the androgen-receptor gene has been reported.9
Androgen is necessary for progression of androgenetic alopecia, as it is not found in males castrated prior to puberty. The progression of androgenetic alopecia is stopped if postpubertal males are castrated. Androgenetic alopecia is postulated to be a dominantly inherited disorder with variable penetrance and expression. However, it may be of polygenic inheritance. It has been noted that follicles from balding areas of persons with androgenetic alopecia are able to produce terminal hairs when implanted into immunodeficient mice.10 This suggests that systemic or external factors may play a role in androgenetic alopecia. Interestingly, female androgenetic alopecia has been reported in a patient with complete androgen insensitivity syndrome. This suggests that factors other than direct androgen action contribute to patterned hair loss.11
As reported in 2005, it was noted in adult mouse skin that the hedgehog (Hh) family of intercellular signaling proteins can stimulate the transition from the resting (telogen) state to the growth phase (anagen) of the hair cycle.12 Whether this will be helpful in the treatment of androgenetic alopecia remains to be seen.
As to the question of whether iron deficiency plays a role in female pattern hair loss, a study by Olsen et al indicated iron deficiency is common in women but is not significantly increased in patients with female patterns of hair loss or chronic telogen effluvium when compared with control subjects
Laboratory Studies
- The most important aspects are the history and the physical examination. In the case of a woman, if virilization is evident, laboratory analysis of dehydroepiandrosterone (DHEA)-sulfate and testosterone may need to be obtained. Some authors have suggested that total testosterone level alone may be adequate to screen for a virilizing tumor. If a thyroid disorder is suspected, obtaining a thyrotropin level is indicated.
- If telogen effluvium is present, laboratory analysis of serum iron levels or a biopsy to note an underlying papulosquamous disorder may be indicated. Telogen effluvium may accelerate the course of pattern alopecia. Iron deficiency is a common and reversible cause of telogen effluvium. A normal CBC count does not exclude iron deficiency as a cause of hair loss. While a low ferritin level is always a sign of iron deficiency, ferritin behaves as an acute phase reactant, and levels may be normal despite iron deficiency. Iron, total iron-binding capacity, and transferrin saturation are inexpensive and sensitive tests for iron deficiency.
- Diffuse alopecia areata may mimic pattern alopecia. The presence of exclamation point hairs, pitted nails, or a history of periodic regrowth or tapered fractures noted on hair counts suggests the diagnosis of diffuse alopecia areata.
- Schmidt et al used dermoscopy to study androgenetic alopecia. They noted brown peripilar casts and miniaturized hairs.16
Procedures
- A biopsy is rarely necessary to make the diagnosis of androgenetic alopecia. If a single biopsy specimen is obtained, it should generally be sectioned transversely if pattern alopecia is suspected. Some dermatopathologists recommend that if a biopsy is to be performed, a sample should be obtained from 2 sites: one for horizontal sectioning and one for vertical sectioning of the hair follicles. Other dermatopathologists point out that one may commonly obtain sufficient information from serial vertical sections to diagnose the condition.
Histologic Findings
In pattern alopecia, hairs are miniaturized. In evolving-pattern alopecia, the diameter of hair shafts varies. Fibrous tract remnants (so-called streamers) can be found below miniaturized follicles. Although androgenetic alopecia is considered a noninflammatory form of hair loss, at times, a superficial, perifollicular, inflammatory infiltrate is noted. A mildly increased telogen-to-anagen ratio is often observed
Treatment
Medical Care
Only 2 drugs currently have US Food and Drug Administration (FDA)–approved indications for treatment of androgenetic alopecia: minoxidil and finasteride.
Minoxidil17
Although the method of action is essentially unknown, minoxidil appears to lengthen the duration of the anagen phase, and it may increase the blood supply to the follicle. Regrowth is more pronounced at the vertex than in the frontal areas and is not noted for at least 4 months. Continuing topical treatment with the drug is necessary indefinitely because discontinuation of treatment produces a rapid reversion to the pretreatment balding pattern.
Patients who respond best to this drug are those who have a recent onset of androgenetic alopecia and small areas of hair loss. The drug is marketed as a 2% or a 5% solution, with the 5% solution being somewhat more effective. A 48-week study compared the 2 strengths in men.18 Findings indicated that 45% more regrowth occurred with the 5% compared with the 2% solution. In general, women respond better to topical minoxidil than men. The increase in effectiveness of the 5% solution was not evident for women in the FDA-controlled studies. Subsequent studies have shown at best a modest advantage to the higher concentration in women. In addition, the occurrence of facial hair growth appears to be increased with the use of the higher-concentration formulation.
Finasteride19
Finasteride is given orally and is a 5-alpha reductase type 2 inhibitor. It is not an antiandrogen. The drug can be used only in men because it can produce ambiguous genitalia in a developing male fetus. Finasteride has been shown to diminish the progression of androgenetic alopecia in males who are treated, and, in many patients, it has stimulated new regrowth.
Although it affects vertex balding more than frontal hair loss, the medication has been shown to increase regrowth in the frontal area as well. Finasteride must be continued indefinitely because discontinuation results in gradual progression of the disorder. A study in postmenopausal women indicated no beneficial effect of the medication in treating female androgenetic alopecia.
Other drugs
Some drugs are not approved by the FDA but are potentially helpful medications.20 In women with androgenetic alopecia, especially those with a component of hyperandrogenism, drugs that act as androgen suppressants or antagonists (eg, spironolactone, oral contraceptives) may be beneficial. Evidence exists of an association between androgenetic alopecia, hypertension, and hyperaldosteronism. Spironolactone could play a dual role in treatment.
Phase III US Food and Drug Administration (FDA) trials of dutasteride to treat androgenetic alopecia are currently on hold. This drug inhibits both type I and type II 5-a reductase isoenzymes and is felt to be 3 times as potent as finasteride in inhibiting the type II enzyme and 100 times as potent in inhibiting the type I enzyme.
Low-level laser light therapy, in particular a red light hairbrush–like device has been marketed as an over-the-counter technique for hair growth. In a double blind, sham-device controlled, multicenter, 26-week trial, 110 patients in the active treatment group who completed the study showed a significantly greater improvement in overall hair regrowth than did the sham group.21 Marketed as the HairMax LaserComb, it has obtained 510K FDA approval for use as a medical device. Note that this approval refers to safety rather than actual efficacy and that the data required for medical devices are quite different from those required to demonstrate the safety and efficacy of drugs.
Androgenetic alopecia is very common; therefore, not surprisingly, it may accompany other forms of hair loss. Cases of telogen effluvium often occur in patients with underlying androgenetic alopecia. Therefore, a search for treatable causes of telogen effluvium (eg, anemia, hypothyroidism), especially in patients with an abrupt onset or a rapid progression of their disease, is indicated.
Surgical Care
Surgical treatment of androgenetic alopecia has been successfully performed for the past 4 decades. Although the cosmetic results are often satisfactory, the main problem is covering the bald area with donor plugs (or follicles) sufficient in number to be effective. Micrografting produces a more natural appearance than the old technique of transplanting plugs.
A 2009 review of surgical procedures concluded that both patients and physicians alike are pleased with the results of contemporary hair transplantation.21 Patients with less than 40 follicular units/cm2 in their donor areas are poor candidates for the procedure. Scalp reduction has been attempted to decrease the size of the scalp to be covered by transplanted hair. However, the scars produced by the reduction technique often spread and become more noticeable with time.
Hair weaving techniques are available, and, together with hairpieces, they offer the patient a prosthetic method of coverage.
.