ALOPECIA AREATA
Epidemiology
At any given time, approximately 0.2 percent of the population has alopecia areata and approximately 1.7 percent of the population experiences an episode of alopecia areata during their lifetime.120,121 However, there are great geographic and ethnic variations in the incidence and prevalence of the disease; this is also seen with respect to the immunogenetic background of patients with alopecia areata. In most patients, the onset is within the first three decades of life although alopecia areata can start at any age. The sex incidence is probably equal.
Etiology and Pathogenesis
Alopecia areata is a chronic, organ-specific autoimmune disease, probably mediated by autoreactive T cells, which affects hair follicles and sometimes the nails. There is an increased frequency of other autoimmune diseases, notably autoimmune thyroid disease in affected adults, and of organ-specific autoantibodies in patients with alopecia areata. Hair follicle autoantibodies are also found in some patients with alopecia areata31,132 although it is unlikely that these autoantibodies are of importance in the primary pathogenesis of alopecia areata.
Studies using human hair follicles transplanted into the skin of immunodeficient mice have provided convincing evidence for a cell-mediated etiology, with a key role for CD8+ T cells, which may recognize a major histocompatibility complex class I-presented autoantigen (possibly expressed during anagen and/or anagen-associated melanogenesis). These experimental data are in line with the concept that a (e.g., interferon-γ-induced) collapse of the normal immune privilege of the anagen hair bulb plays a key role on the primary pathogenesis of the disease. Evidence in support of the concept that melanogenesis-associated autoantigens, which are normally sequestered from immune recognition by a functional hair follicle immune privilege, may be a key target of autoaggressive inflammation in alopecia areata133 is slowly accumulating.137,138 Histologically, alopecia areata is characterized by an inflammatory infiltrate, comprised mainly of T cells, in and around the bulbs of anagen hair follicles . The histopathologic features of alopecia areata, however, are stage-dependent, and the classic features may be missing in subacute and chronic lesions, rendering it prudent to include alopecia areata in the differential diagnosis whenever high percentages of telogen hairs or miniaturized hairs are present, even in the absence of a peribulbar lymphocytic infiltrate.
Anagen follicles attacked by this inflammatory infiltrate move prematurely into catagen, followed by telogen, and then enter a dystrophic anagen status. Most follicles may continue to cycle but, while the disease remains active, are unable to progress beyond an early stage of anagen development and thus do not produce normal hair shafts. An important feature of the pathology is that hair follicles are not destroyed in alopecia areata, possibly because the disease spares the follicular stem cell compartment in the mid-outer root sheath region.
The predisposition to alopecia areata is genetically determined. Between 10 percent and 20 percent of patients with alopecia areata give a family history of the disease, and the true figure is probably higher because mild cases may pass unnoticed or are concealed.124 There are several reports of alopecia areata in twins, some with concurrent onset. One small study of alopecia areata in twins found a concordance of 55 percent in monozygotic twins but none in dizygotic twins. The genetic predisposition is polygenic in nature. To date, most genes found to be associated with alopecia areata are involved in regulating immune responses, yet there are substantial geographic/ethnic differences in the immunogenetics of alopecia areata. The strongest associations have been with genes of the HLA-D region of the major histocompatibility complex locus. There is also an association between severe forms of alopecia areata and polymorphisms in the autoimmune regulator gene on chromosome 21.145 Alopecia areata is common in Down syndrome, and there is also a high frequency of the disease (more than 30 percent) in autoimmune polyendocrinopathy-candidiasis-ectodermal dysplasia syndrome (also called autoimmune polyglandular syndrome-1), a usually autosomal recessive disorder in which there are mutations in the autoimmune regulator gene
A variety of environmental factors, including infection, drugs, trauma, and stress, have been suggested as triggering alopecia areata, although most patients with alopecia areata are unaware of any obvious precipitating factor. It is possible, though hard to prove, that a diversity of insults, physical or psychological, may trigger episodes of alopecia areata128 but there is no evidence that they influence the prognosis.
Clinical Features
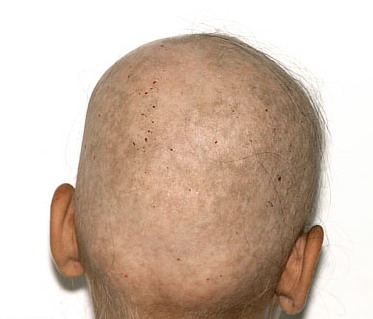
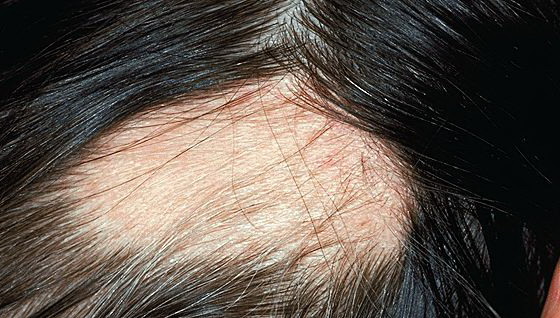
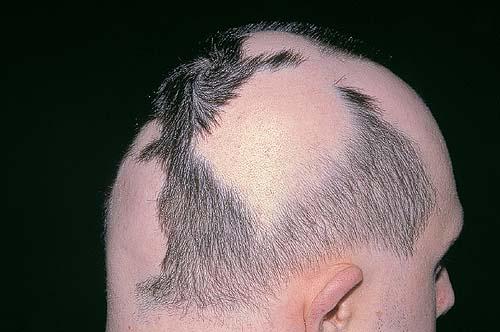
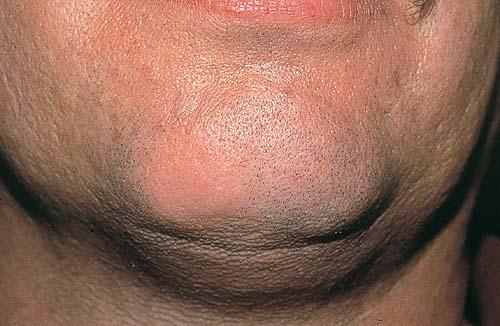
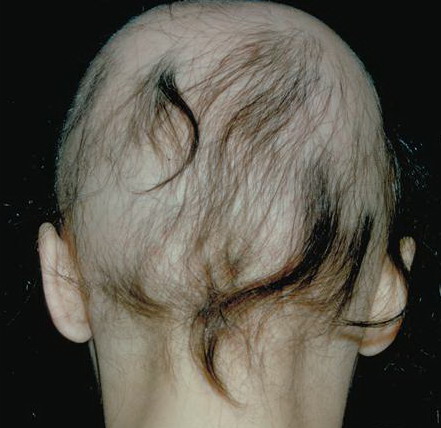
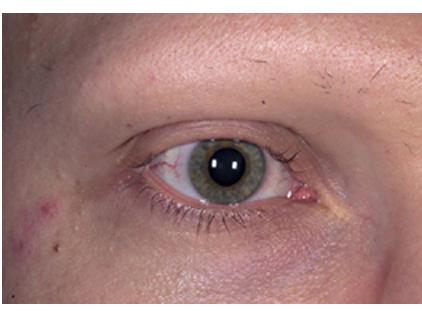
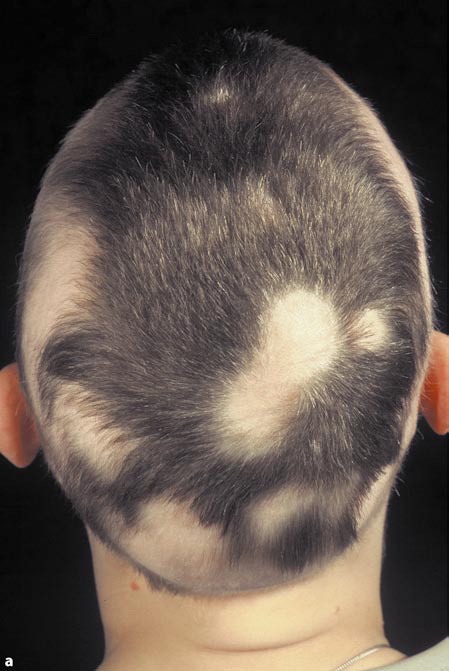
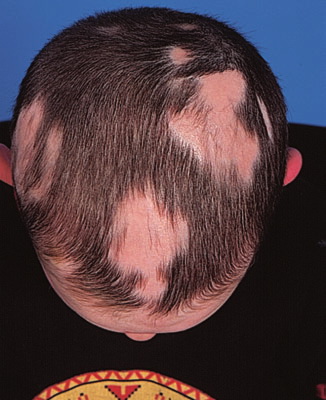
Alopecia areata typically presents with round patches of hair loss. Patches may be single or multiple, and may coalesce . Although most obvious on the scalp, any hair-bearing skin can be affected, and is frequently found to involve the beard area. The term alopecia totalis is used to describe complete loss of terminal hair on the scalp and alopecia universalis to describe total loss of all terminal hair on the scalp and body.148 Ophiasis refers to a band-like pattern of hair loss at the periphery of the scalp . The scalp usually appears normal. The pathognomonic “exclamation mark” hairs may be present, particularly at the periphery of areas of hair loss . These short broken hairs, whose distal ends are broader than the proximal ends, illustrate their inherent sequence of events: follicular damage in anagen and then a rapid transformation to telogen. White or graying hairs are frequently spared and probably account, in cases of fulminant alopecia areata, for the mysterious phenomenon of “going gray overnight” . Nails in patients with alopecia areata may show fine pitting or, less commonly, mottled lunula, trachyonychia, or onychomadesis .
Differential Diagnosis
Though the clinical diagnosis is usually straightforward, other conditions that typically need to be considered are:
· Tinea capitis. Obvious inflammation (e.g., scaling, pustules) in association with patchy hair loss suggests a diagnosis of tinea capitis and excludes alopecia areata.
· Trichotillomania. This can be difficult to distinguish from alopecia areata (and may, in fact, be associated with it, especially in children). However, here the hair loss is rarely complete and the broken hairs are usually firmly anchored in the scalp, unlike exclamation point hairs. A biopsy may be needed.
· Early scarring alopecia.
· Syphilis (alopecia areolaris).
Diffuse alopecia areata can be difficult to differentiate from other causes of diffuse hair loss, and may be associated with them (e.g., thyroid abnormalities, other autoimmune diseases and syphilis). Diffuse alopecia areata usually progresses rapidly and the diagnosis becomes clear with time, but a biopsy may be necessary to clarify remaining uncertainties.
Prognosis
Spontaneous remission can be expected in the majority of cases where hair loss is limited to a few small patches (possibly, up to approximately 80 percent within 1 year), although most patients experience recurrences at some stage.149 The prognosis in extensive alopecia areata, particularly alopecia totalis and universalis, is less favorable and fewer than 10 percent of patients in the latter two groups recover spontaneously. The ophiasis pattern of alopecia also tends to be recalcitrant. Other features pointing to a poor prognosis include onset in childhood, loss of body hair, nail involvement, atopy, and a positive family history for alopecia areata.
Management
Counseling of patients on the nature of alopecia areata, its prognosis, and the treatment options is essential. For the majority of patients, alopecia areata is a cosmetic issue. Occasionally, it causes physical disability (e.g., when there is eyelash involvement or marked nail dystrophy). Nevertheless, the cosmetic importance of hair is such that alopecia areata can cause severe emotional problems, particularly in children and young women, though by no means restricted to these groups.2 In view of the limited efficacy of current forms of treatment, the physician has an important role in helping patients adapt to their lack of hair. This is not an easy task and input from other health professionals, such as a clinical psychologist, may be needed. Many patients are helped by involvement in patient support groups. With children, it is often the parents whose reactions must be addressed for the child to adjust to the hair loss. The National Alopecia Areata Foundation (http://www.naaf.org) is an excellent source of information for patients.
Treatment
There is relatively little evidence from well-designed clinical trials, and so treatment recommendations are based mainly on case series and clinical experience (Box 86-1).150 Helpful guidelines for managing alopecia areata have been developed.4,6
Box 86-1 Treatment of Alopecia Areata
· Patchy alopecia
o Intralesional corticosteroids: Up to 2 mL injected/session and repeated at intervals.
o Potent topical steroid 1-2×/day.
o Topical anthralin 0.1%-2.0% once daily. Wash off after 10-20 min, steadily increase contact duration, switch to higher dose if no significant irritation.
o Minoxidil lotion (5%) twice daily.
· Extensive or rapidly progressive alopecia.
o Contact immunotherapy.
o Systemic corticosteroids. Benefits are uncertain and must be weighed against risk of systemic corticosteroid therapy.
o Wig or hairpiece.
· Alopecia totalis/universalis
o Contact immunotherapy.
o Topical/systemic steroids.
o Wig or hairpiece.
CONSERVATIVE MANAGEMENT
All of the currently available treatments for alopecia areata have a high failure rate and none alters the natural history of the disease. After discussion of the options patients may therefore opt not to be treated, other than to wear a wig if appropriate. ‘No treatment’ is a legitimate option in patients with a short history and limited disease, in view of the high rate of spontaneous remission in this group.
TOPICAL CORTICOSTEROIDS
Topical corticosteroids are widely used to treat alopecia areata. There is some evidence of efficacy if potent corticosteroids are used under occlusion, but less aggressive treatment regimens are probably ineffective.
INTRALESIONAL
CORTICOSTEROIDS
Intralesional corticosteroids are the most effective approach for treating patchy alopecia areata. Hydrocortisone acetate (25 mg/mL) and triamcinolone acetonide (5 to 10 mg/mL) are commonly used, either by subdermal injection or using a needle-less device. Multiple injections repeated monthly are usually necessary, limited by patient discomfort. Intralesional corticosteroids are not appropriate in rapidly progressive or extensive disease. Especially with triamcinolone injections, there is a significant risk of inducing skin atrophy, which may increase exponentially with each repeated injection.
SYSTEMIC
CORTICOSTEROIDS
Oral corticosteroid therapy can induce short-term hair regrowth in patients with alopecia areata; however, hair regrown is usually lost after treatment is discontinued. Newer regimens that involve pulsed oral corticosteroids (e.g., prednisolone 200 mg once weekly for 3 months or dexamethasone 5 mg daily for 2 consecutive days/week for 3 months) may also induce hair regrowth in some patients. No significant side effects have been reported in published series but cannot be ruled out, and long-term benefits have not been shown.
TOPICAL MINOXIDIL
SOLUTION
There is limited clinical trial evidence that topical minoxidil solution (TMS) stimulates hair regrowth in some patients.3,157 Minoxidil is ineffective in alopecia totalis/universalis.
ANTHRALIN
Data from small case series suggest that treatment with anthralin cream is helpful in some cases, but the overall response rate is low.158 However, especially in children where steroids or contact immunotherapy are decided against, this is a reasonable and safe treatment option.
PHOTO(CHEMO)THERAPY
Phototherapy using UVB has been widely used, but there is no convincingly documented evidence of efficacy. Some case series have reported success using psoralen and UVA light (local or whole body), but there have been reports of high relapse rate when treatment is discontinued. Retrospective reviews have suggested that the response is no better than that expected from the natural history. The deleterious long-term effects of phototherapy-induced premature skin aging and photocarcinogenesis argue against this treatment option, especially in children.
CONHERAPYTACT IMMUNOT
In addition to intralesional glucocorticoid injections, this is the only form of therapy for which efficacy has been convincingly documented. This may be the most effective treatment for patients with extensive alopecia areata, although it is not widely available. Also, there is insufficient comprehensively comparative analysis with alternative treatment options. The patient is sensitized to a potent allergen [usually diphenylcycloprenone (DPCP) or squaric acid dibutylester (SADBE)] and then a solution of DPCP or SADBE is painted on the scalp once weekly. The concentration of DPCP or SADBE is adjusted to induce a mild dermatitis reaction. Published response rates vary widely (9 percent to 85 percent) but clinical experience suggests that approximately 30 percent of patients with extensive alopecia areata achieve a cosmetically worthwhile response after 6 months of treatment. Continuous or intermittent treatment is needed to maintain the response in most patients. Alopecia totalis/universalis is less likely to respond to contact immunotherapy, and it is unclear whether patients with rapidly progressive disease profit.
Risks include severe dermatitis, urticaria, and pigmentary abnormalities including vitiligo (an important consideration in racially pigmented skin). Sensitization of health care workers and relatives handling the immunogen is also a significant hazard. Contact immunotherapy has been in use since the early 1980s, and no long-term side effects have been reported.
COSMETIC MEASURES
Female patients with extensive alopecia areata often choose to wear a wig or hairpiece. Hair weaves can give good results if sufficient hair remains, although they are expensive to maintain. Locks of Love (http://www.locksoflove.org) is an organization that collects human hair and provides hairpieces to financially disadvantaged children younger than age 18 years with alopecia areata and other chronic forms of alopecia. Wigs are generally less successful in men where other hair styles, such as shaving the scalp, are often a more acceptable approach. Temporary tattooing can be helpful for loss of eyebrows.