| Atypical fibroxanthoma =صفروم ليفي غير نموذجي |
|
|
▪ ATYPICAL
FIBROXANTHOMA
Epidemiology
Atypical fibroxanthoma (AFX) is a relatively common rapidly growing neoplasm of intermediate malignant potential. It occurs mainly on sun-exposed skin (face, neck, and hands) of elderly individuals. The male-to-female ratio is essentially equal. AFX has been reported in the second to tenth decade, with a mean age of approximately 69 years. Etiology and Pathogenesis The anatomic distribution and the presence of cyclobutane pyrimidine dimers support a pathogenic role for ultraviolet radiation in the development of AFX. Tumors may occur 10 to 15 years after local ionizing irradiation. Clinical Findings
HISTORY
The patient may report a lesion on sun-damaged skin of relatively rapid onset. The lesion usually presents as a solitary, often dome-shaped nodule, which may be eroded or ulcerated. The size of presentation is usually less than 3 cm in diameter.
CUTANEOUS LESIONS
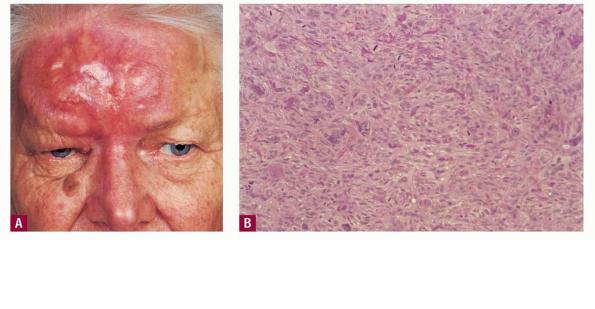
AFX appears as an asymptomatic, solitary papule or nodule often resembling a squamous cell carcinoma, basal cell carcinoma, or even a necrotic pyogenic granuloma. It is often friable, eroded, or ulcerated. The AFX is typically less than 2 cm in size and is most commonly seen on the actinically damaged skin of older patients, especially ears, cheeks, nose, and scalp. The background skin is often sun damaged. AFX may be found in the setting of other non-melanoma cutaneous malignancy.
LABORATORY TESTS
Histopathology. Diagnosis is by skin biopsy. Specimens often show partially exophytic tumors with ulceration of the overlying epidermis. A grenz zone may be present, but usually the tumor abuts onto the dermal-epidermal
Special Tests . Immunohistochemically, AFX has variable profiles, but cells usually express vimentin and histiocytic markers such as α1-antitrypsin, α1-antichymotrypsin, HAM-56 antigen, and CD68. A few express factor XIIIa. CD99 has been proposed to be a relatively sensitive marker (73 percent of cases) and, in context, a specific marker for these tumors. Expression of S100A6 also appears to be a sensitive marker for AFX. MIB1 (Ki-67) may be another useful marker in this highly proliferative tumor. LN2 (CD74) has been suggested to represent a marker of more aggressive behavior in this tumor. Prognosis and Clinical Course AFX has long been regarded as a neoplasm with extremely low metastatic potential. There have been several reports of metastatic disease, some resulting in death.7 Many consider AFX to be a superficial variant of malignant fibrous histiocytoma (MFH), which has much more ominous behavior. Overlap between these two tumors may account for the AFX cases with reported metastases. AFX is often found in the setting of diffuse actinic damage and other non-melanoma skin cancer, so close follow-up after complete tumor extirpation is prudent.
Treatment
Treatment for AFX is surgical. Studies have suggested that Mohs micrographic surgery provides a lower rate of recurrence than wide local excision. Excision should be to the level of the deep subcutaneous tissue. Adjuvant treatment with radiation may be considered for tumors with particularly aggressive onset. It also may be considered in the setting of positive LN2 (CD74) staining of the tumor. Prevention Protection from ultraviolet damage may serve as one measure of prevention of this tumor.
|