| Xanthogranuloma_Juvenile = الحبيبوم الاصفر الفتوي |
|
|
JUVENILE
XANTHOGRANULOMA
Clinical Findings
CUTANEOUS LESIONS
JXG is a benign, self-healing disorder that is characterized by asymptomatic yellowish papulonodular lesions of the skin and other organs in the absence of a metabolic disorder. Lesions consist of an infiltrate of histiocytes with a progressively greater degree of lipidation.
In JXG two main clinical forms can be distinguished, a papular and a nodular form. In both the lesions are initially orange-red or red-brown but quickly turn yellowish. The papular form is characterized by numerous (up to
RELATED PHYSICAL FINDINGS
Ocular involvement is the most typical extra-cutaneous manifestation. It may precede or follow the cutaneous lesions. Ocular JXGs are usually unilateral and
Laboratory Tests
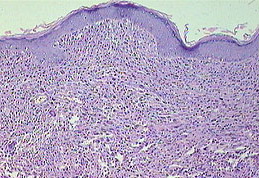
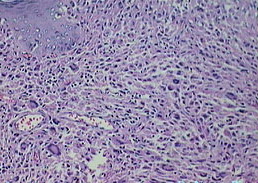
No abnormalities in laboratory test results are usually found in JXG except in the very rare cases in which juvenile chronic myeloid leukemia is associated with JXG. Histopathologic and Ultramicroscopic Findings Biopsy sections of JXG lesions show a feature that is common to many NLCHs, that is, a nonepidermotropic histiocytic infiltrate lacking Langerhans granules. Early lesions of JXG are characterized by a monomorphous, non-lipid-containing histiocytic infiltrate that occupies at least the upper half, and sometimes the entire thickness, of the dermis. Mature lesions contain foam cells, foreign-body giant cells, and Touton giant cells, mainly distributed in the superficial dermis and on the border of the infiltrate. Lymphocytes, eosinophils, and neutrophils are variably associated. Older lesions may show fibrosis. In mature lesions, fat stains yield positive results. The majority of JXG lesional biopsy sections stain positive for CD68/Ki-M1P and factor XIIIa but negative for CD1a and S100 protein. Under the electron microscope, the histiocytes that characterize the early stage of the disease exhibit pleomorphic nuclei, are rich in pseudopods, and contain many elongated and irregular dense bodies. Clusters of comma-shaped bodies can occasionally be observed. In older lesions, there is a predominance of foam cells, the cytoplasm of which is completely filled with lipid vacuoles, cholesterol clefts, and myeloid bodies. Touton giant cells are extremely large and sometimes contain more than 10 nuclei. Lipid material fills the periphery, whereas mitochondria and lysosomes predominate at the center. The lesions of PX are composed almost entirely of foam cells and Touton giant cells. There is no evidence of a primitive histiocytic phase, and inflammatory cells are scarce or absent. Ultrastructurally, the cytoplasm is completely filled with lipid vacuoles without a limiting membrane, myeloid bodies, and lysosomal inclusions. Comma-shaped bodies are not found in these histiocytes. Differential Diagnosis The differential diagnosis of JXG is summarized in Box 149-1. Complications Eye involvement of a JXG lesion can cause a major visual problem leading to
Box 149-1 Differential Diagnosis of Juvenile Xanthogranuloma
Prognosis and Clinical Course The cutaneous lesions of JXG tend to flatten with time. Each lesion evolves separately; thus, lesions at different stages of development may be seen in the same patient. Both cutaneous and visceral lesions disappear spontaneously, usually within 3 to 6 years. The patient's general health is not impaired, and physical and mental development is normal. Metabolic disturbances have not been identified. In the absence of associated conditions, prognosis is good. |