Tungiasis
Tungiasis is an infestation by the burrowing flea Tunga penetrans or related species. The flea has many common names as listed above. Tungiasis was first reported in crewmen who sailed with Christopher Columbus. The flea is indigenous to the West Indies/Caribbean/Central America region, but it has spread to Africa, India, Pakistan, and South America. Travelers to endemic areas may import cases to other countries, including the United States. These painful infections can cause significant morbidity in groups, such as soldiers.
To reproduce, the flea requires a warm-blooded host. In addition to humans, reservoir hosts include pigs, dogs, cats, cattle, sheep, horses, mules, rats, mice, and other wild animals.
Pathophysiology
The main habitat is warm, dry soil and sand of beaches, stables, and stock farms. Upon contact, the fleas invade unprotected skin. The most common site of involvement is the feet (interdigital skin and subungual area). The flea has limited jumping ability.
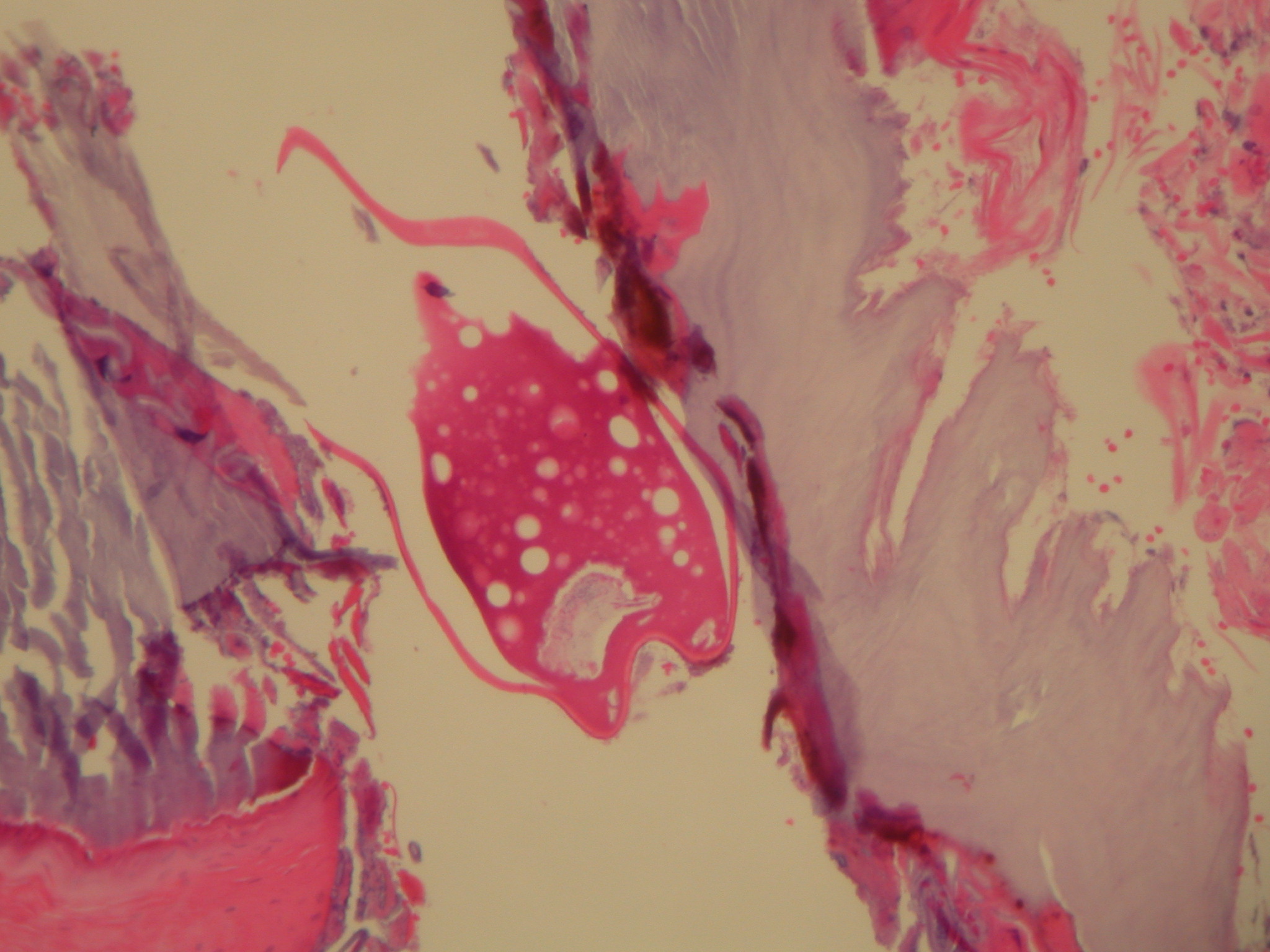
Both the male and the nonfertilized female flea feed intermittently on warm-blooded hosts. Once impregnated, however, the female flea anchors herself to the skin by using biting mouthparts and burrows into the epidermis. Because the process is painless, a keratolytic enzyme may be involved. The flea expands, often reaching 1 cm in diameter. The head is down into the upper dermis feeding from blood vessels, while the caudal tip of the abdomen is at the skin surface, often forming a punctum or an ulceration. The flea breathes through this opening. In many cases, this is described as a white patch with a black dot.
Over 1-2 weeks, more than 100 eggs, which fall to the ground, are individually released from this exposed orifice. Afterwards, the flea dies and is slowly sloughed by the host. The eggs hatch on the ground in 3-4 days, go through larval and pupal stages and become adults in 2-3 weeks. The complete life cycle lasts approximately 1 month.
Imported cases rarely occur in the United States.6,7
In the endemic areas, the prevalence ranges from 15-40%, but cases in other areas are sporadic. Six percent of the patients visiting a travel-associated dermatosis clinic in Paris had tungiasis.5
Individual lesions may be painful, although sometimes they are pruritic or even asymptomatic. In most cases, tungiasis resolves without complications. However, heavy infestations may lead to severe inflammation, ulceration, and fibrosis. The risk of secondary infection is high. Lymphangitis, gangrene, and ainhum may occur. Death from tetanus associated with tungiasis has been reported.
Lesions can range from asymptomatic to pruritic to extremely painful.
The typical presentation is a nodule (usually on the foot) that slowly enlarges over a few weeks in a patient who has recently been in an endemic area. The nodule can range from 4-10 mm in diameter.
Tungiasis is caused by an infestation with the burrowing flea T penetrans.
Treatment
Reported topical treatments include cryotherapy or electrodesiccation of the nodules. Application of formaldehyde, chloroform, or dichlorodiphenyltrichloroethane (DDT) to the infested skin has been used, but it may cause a person's own morbidity. Topical ivermectin, metrifonate, and thiabendazole have also been reported as effective. Occlusive petrolatum suffocates the organism. Twenty-percent salicylated petroleum jelly (Vaseline) applied 12-24 h in profound infestations caused the death of the fleas and facilitated their manual removal.9 These treatments do not remove the flea from the skin, and they do not result in quick relief from painful lesions. The flea may also be gently removed with a needle or a forceps.
Surgical Care
A number of surgical treatment methods are available. The flea can be removed from its cavity with sterile instruments, but this is more difficult when the flea is engorged. The orifice needs to be enlarged, and the entire nodule should be curetted or excised. An antibiotic ointment may be applied, along with systemic antibiotic therapy when indicated. Aggressive treatment of secondary infection and tetanus prophylaxis are important.
Usually, topical and/or surgical modalities are used to treat tungiasis; however, a report relates oral niridazole clearing cases in patients who were infested. Oral ivermectin was found to be ineffective in at least one study.
Parasite biochemical pathways are sufficiently different from the human host to allow selective interference by chemotherapeutic agents in relatively small doses. A combination of direct toxic action on the flea and anti-inflammatory action on the surrounding tissue is postulated.