|
Pyoderma Gangrenosum = تقيح الجلد المواتي |
 |
 |
 |
|
Pyoderma Gangrenosum
First described in 1930 , pyoderma gangrenosum was once considered pathognomonic of idiopathic ulcerative colitis but has since been described in association with a wide variety of disorders, including roughly 5% of
|
|
patients with Grohn's disease. Beginning as folliculocentric pustules or fluctuant nodules, the lesions ulcerate and have sharply circumscribed violaceous, raised edges in which necrotic pustules may be seen. The disease most commonly occurs on the lower extremities and trunk in adults who are 30 to 50 years old. Occasionally it occurs in childhood, affecting the buttocks, perineal region, and head and neck area . Koebnerization occurs at sites of trauma, including intravenous puncture sites, surgical wounds, and peristomal sites . Roughly 70% of cases are associated with inflammatory bowel disease, hematologic disorders including acute lymphoid and myeloid leukemias and myeloma, rheumatologic conditions including rheumatoid arthritis and lupus erythematosus, and hepatopathies , including chronic active hepatitis, primary biliary cirrhosis, and sclerosing cholangitis . Both a superficial granulomatous variant and a vesiculopustular variant comprising disseminated vesicles and necrotizing pustules, some follicular based, have been observed without accompanying systemic disease. The vesiculopustular variant has also been seen in association with ulcerative colitis and/or underlying liver disease . Pyoderma gangrenosum has been associated with the administration of drugs including interferon (IFN}-a in the setting of chronic granulocytic leukemia, the antipsychotic agent sui pride , granulocyte colony-stimulating factor , the epidermal growth factor-tyrosine kinase inhibitor gefitinib (lressa) , the retinoid isotretinoin , and the thionamide propylthiouracil .
|
|
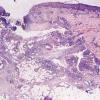
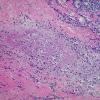
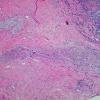
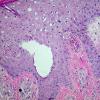
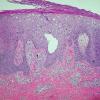
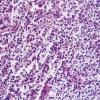
Histopathology
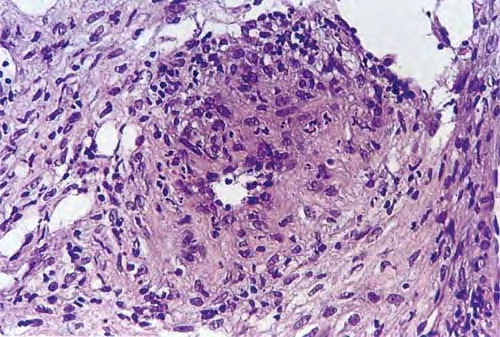
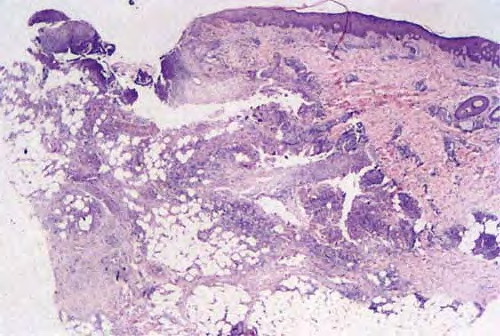
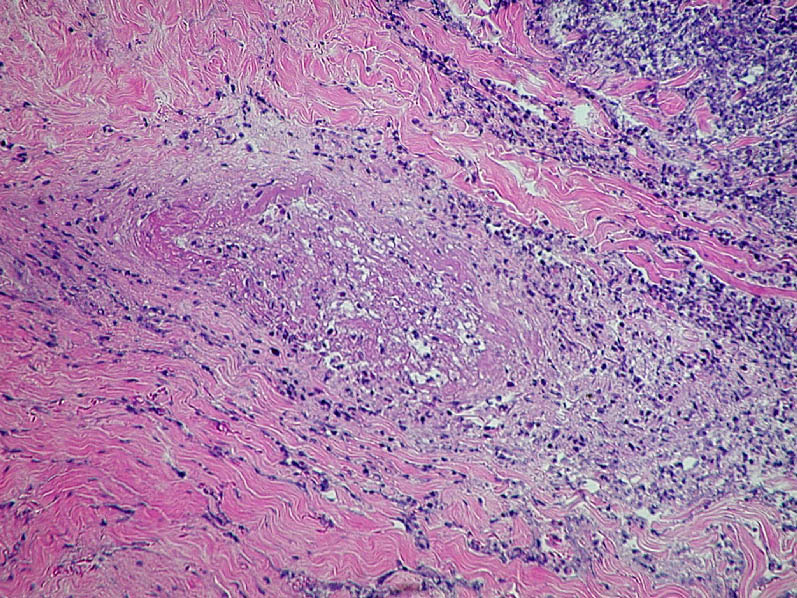
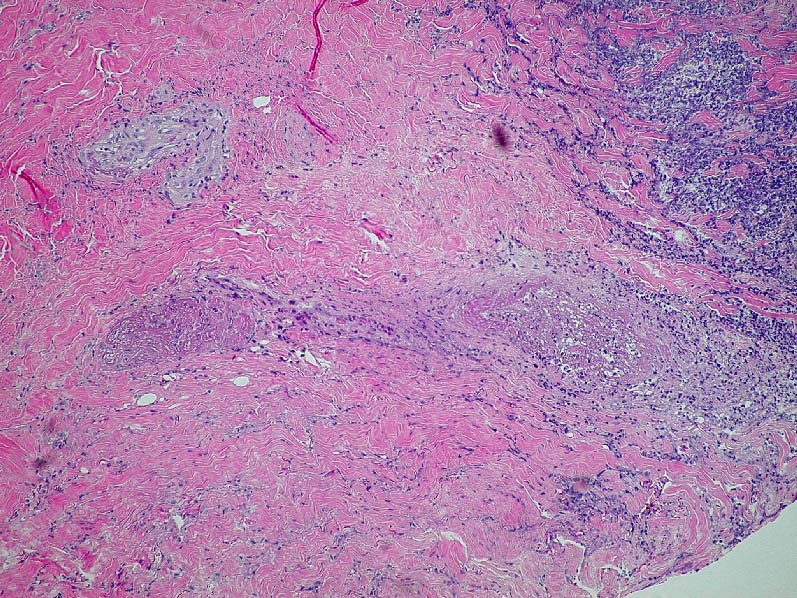
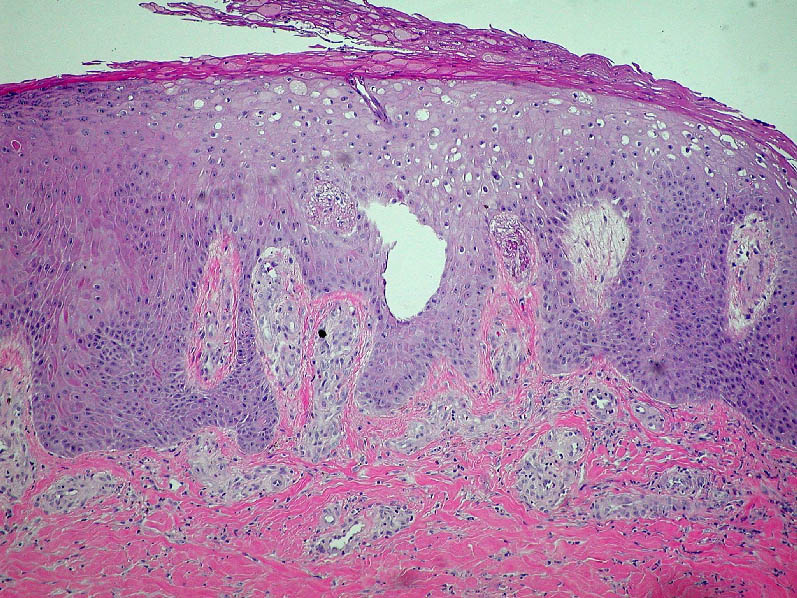
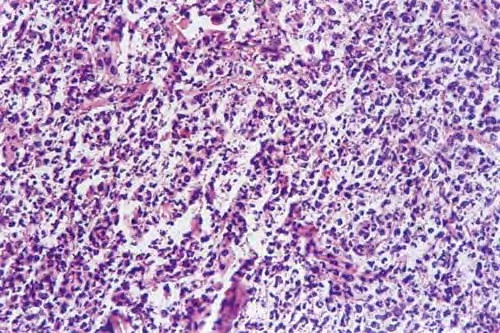
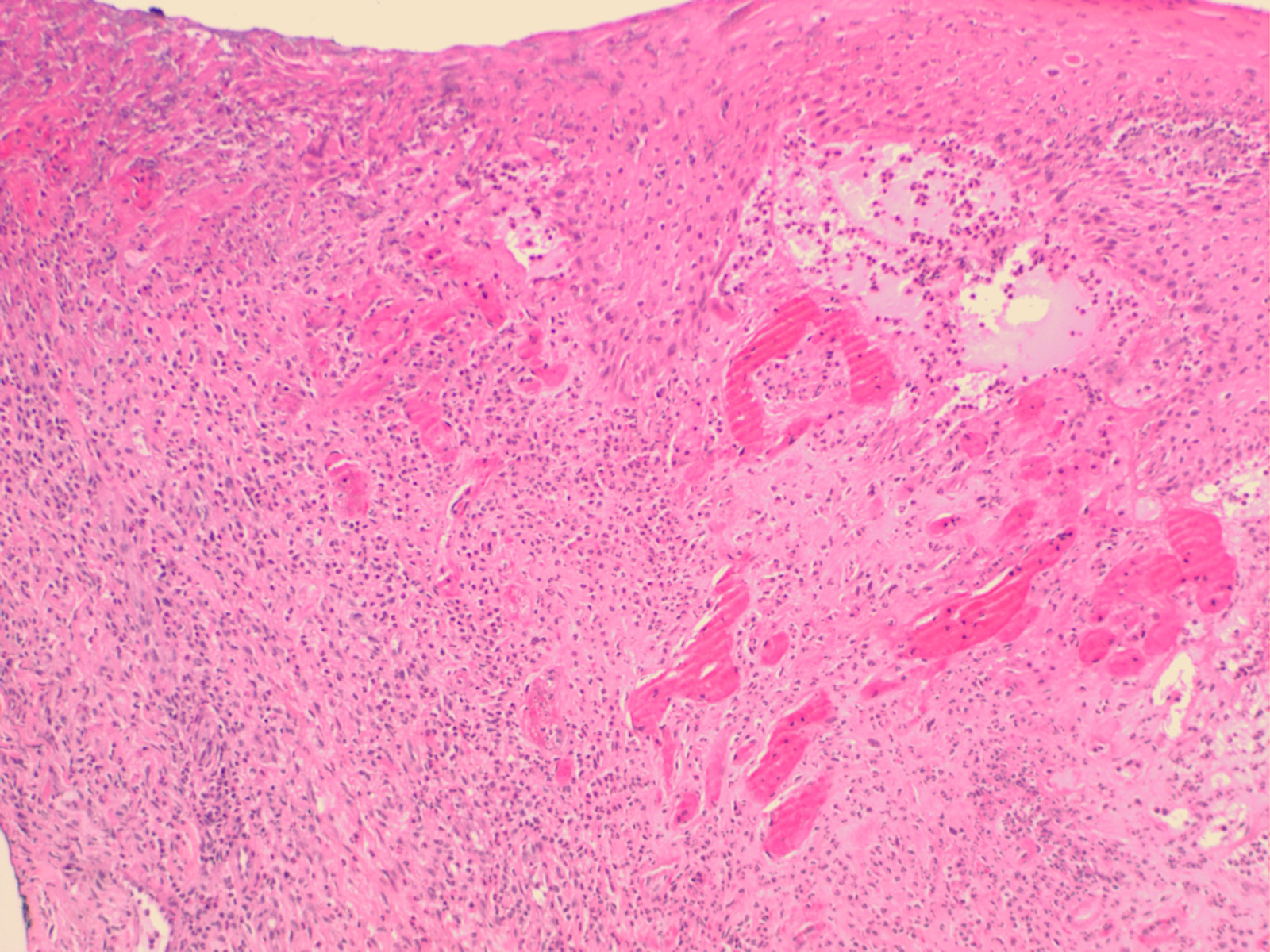
. Pyoderma gangrenosum exhibits a dichotomous tissue reaction, showing central necrotizing suppurative inflammation, usually with ulceration, and a peripheral lymphocytic vascular reaction comprising perivascular and intramural lymphocytic infiltrates, usually without fibrin deposition or mural necrosis . Transitional areas show neutrophils in a loose cuff around the angiocentric lymphocytic infiltrates, defining a mixed lymphocytic and neutrophilic vascular reaction termed a Sweet's-Iike vascular reaction . Bullous lesions may also demonstrate a Sweet's-like vascular reaction with perivascular disintegrating
neutrophilic infiltrates and hemorrhage without mural necrosis or luminal fibrin deposition. At variance with Sweet's syndrome is destruction of the connective tissue framework with resultant tissue pathergy . Although a leukocytoclastic vasculitis may be observed in areas of maximal tissue pathology, pyoderma gangrenosum does not reflect a primary vasculitis . In some cases a necrotizing pustular follicular reaction may be the central nidus of the lesion, particularly in the vesicular pustular variant associated with ulcerative colitis or hepatobiliary disease. In the superficial granulomatous variant, florid pseudoepitheliomatous hyperplasia may be observed along with the intraepithelial and superficial dermal suppurative granulomatous inflammation with admixed plasma cells and eosinophils . Gases of pyoderma gangrenosum associated with Grohn's disease may have areas of granulomatous inflammation .
|
|
Differential Diagnosis. Tissue neutrophilia with epithelial undermining and ulceration in the absence of leukocytoclastic vasculitis, fungal, bacterial, or mycobacterial organisms (which, if indicated, may be demonstrable with culture and special stains, e.g., periodic acid-Schiff, Gomori methanamine
|
|
silver, Brown and Brenn, Gram's, Ziehl-Neelson, and auramine-rhodamine preparations), strongly implicates pyoderma gangrenosum when seen in the appropriate clinical setting . An incipient lesion of pyoderma gangrenosum, however, may be indistinguishable from Sweet's syndrome, although the latter is rarely folliculocentric and does not show lysis of dermal collagen or vessel wall necrosis in areas of maximum dermal neutrophilia. In addition, clinical features usually make the distinction possible. Because of prominent follicular involvement, the differential diagnosis should also include other causes of necrotizing pustular follicular reactions with an accompanying vasculopathy, such as mixed cryoglobulinemia, Behcet's disease, rheumatoid vasculitis,
|
|
herpetic folliculitis, acute pustular bacterid, and pustular drug reactions . These other conditions frequently have a necrotizing mononuclear cell or neutrophil predominant vasculitis in contrast to the non necrotizing vascular reaction of pyoderma gangrenosum. Other causes of a Sweet's-like vascular reaction include the bowel arthritis dermatosis syndrome, Behcet's disease, idiopathic pustular vasculitis, rheumatoid arthritis, acute pustular bacterid, and Sweet's syndrome .
|
|
Pathogenesis. Direct immunofluorescence testing supports a vasculopathy by virtue of perivascular deposition of immunoreactants, mainly immunoglobulin {Ig} M and C3 , in more than half of patients. This change occurs in nonspecific vessel injury and does not support a humoral-based pathogenesis. Defective cell-mediated immunity without humoral abnormalities has been implicated in some patients . Immunoelectrophoresis has revealed a monoclonal gammopathy, most commonly of the IgA type, in 10% of patients with pyoderma gangrenosum . A recent polymerase chain reaction analysis demonstrated that patients with pyoderma gangrenosum have clonal expansions of T cells in the peripheral blood and skin. These clonal expansions are shared between both sites, suggesting that T cells are trafficking to the skin under the influence of an antigenic stimulus . In further support of a potential antigenic stimulus, patients with pyoderma gangrenosum have elevated levels of interleukinB {IL-B}, a powerful neutrophilic chemoattractant, in both the serum and fibroblasts of affected skin .
|
|
|
|
|