|
Pemphigus Vulgaris
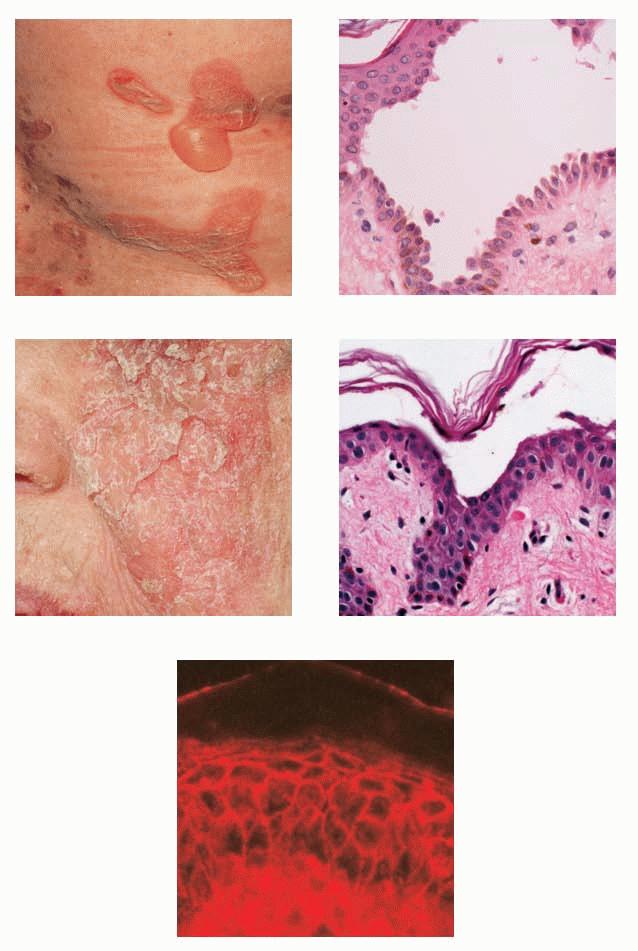
Pemphigus vulgaris develops primarily in older individuals, presenting with large and flaccid bullae. They break easily and leave denuded areas that tend to increase in size by progressive peripheral detachment of the epidermis, leading in some cases to widespread cutaneous involvement. The lesions characteristically involve the oral mucosa, scalp, midface, stemum, groin, and pressure points. Oral lesions are almost invariably present and may be the first manifestation of the disease (10% of cases) . Before corticosteroids became available, the mortality of this disease was high because of fluid loss and superinfection.
Histopathology.
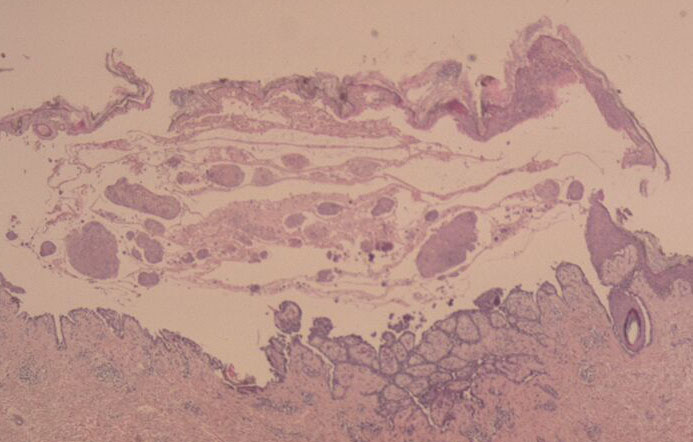
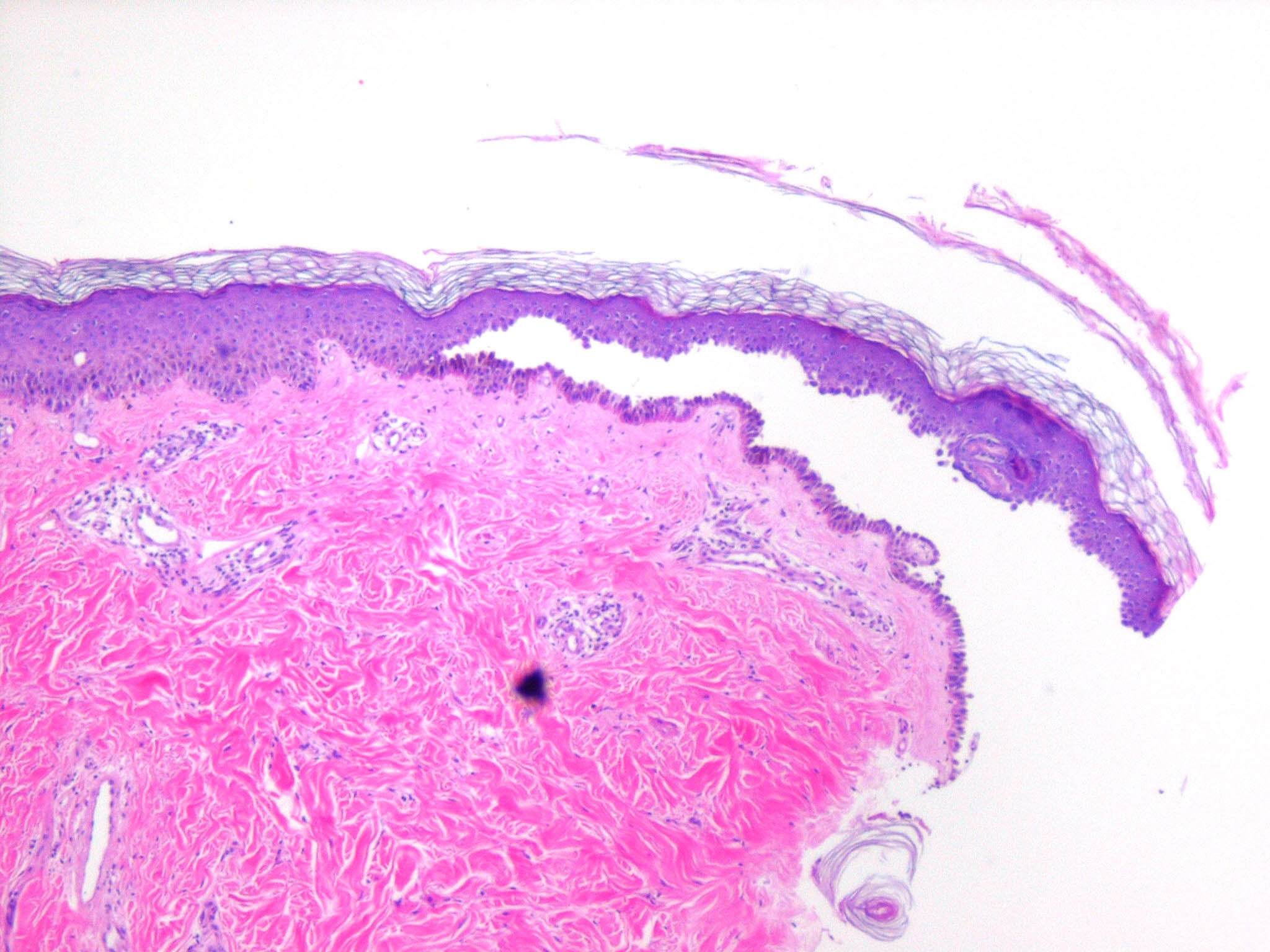
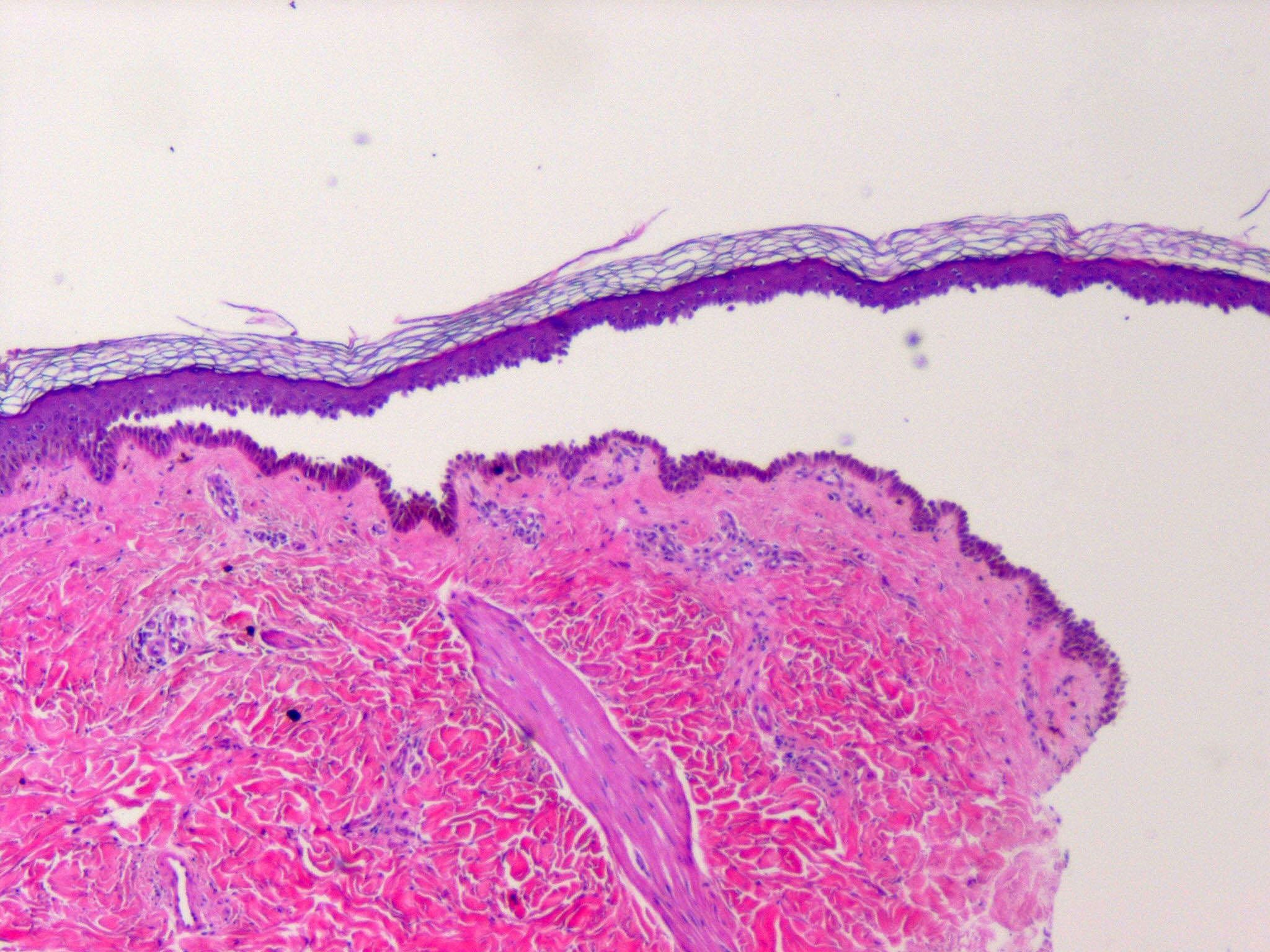
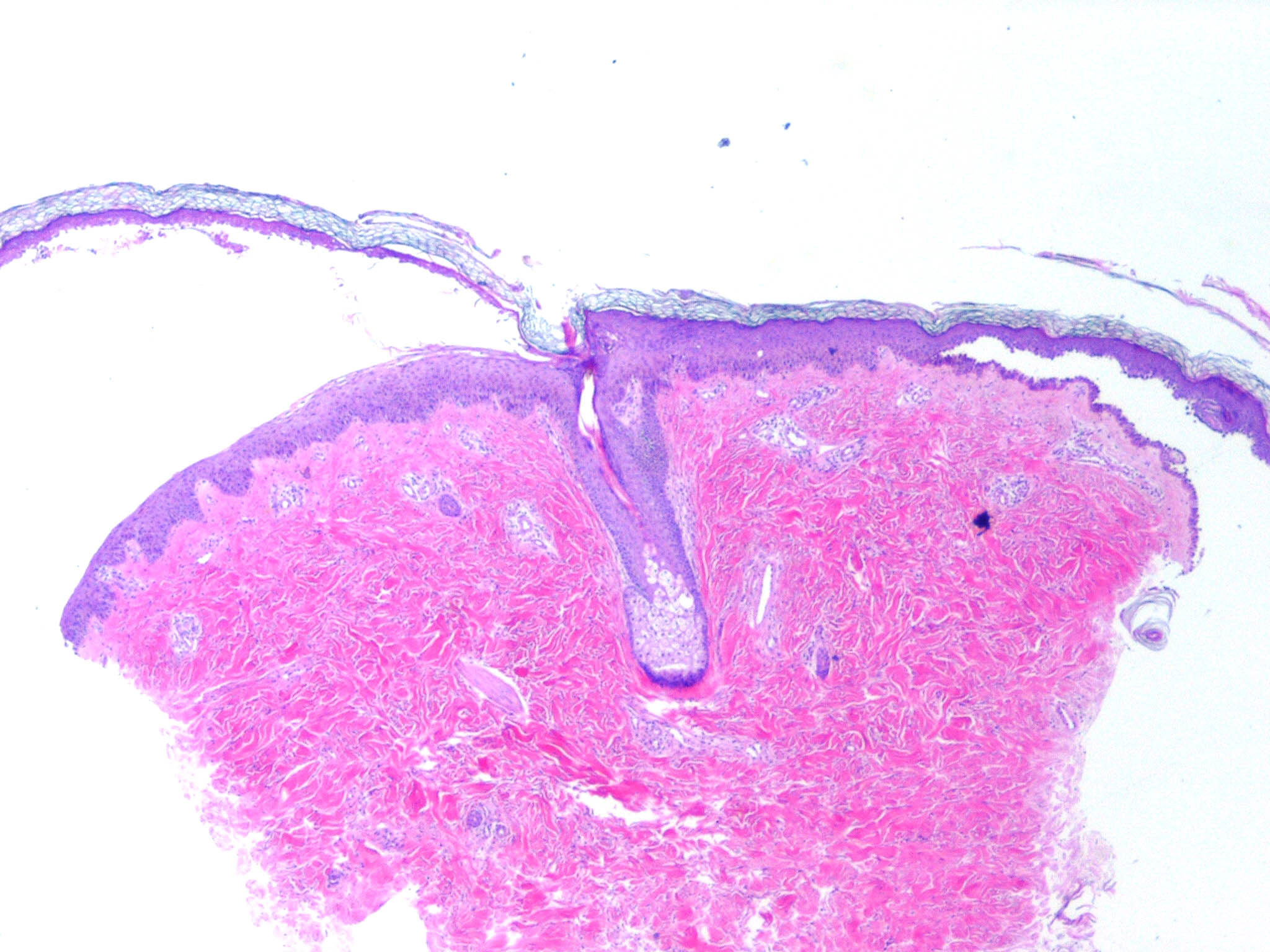
It is important that early blisters, preferably small ones, are selected for biopsy. Care should be given to keeping the epidermis attached to the dermis because the torque applied in punch biopsies may separate the blister roof from the blister base. Therefore, a refrigerant spray may be used before excising the blister with a punch biopsy, or it may be excised with a scalpel. If no recent blister is available, an old one may be moved into the neighboring skin by gentle vertical pressure with a finger (positive Asboe-Hansen sign). The newly created cleavage will reveal early and specific histologic changes.
|
|
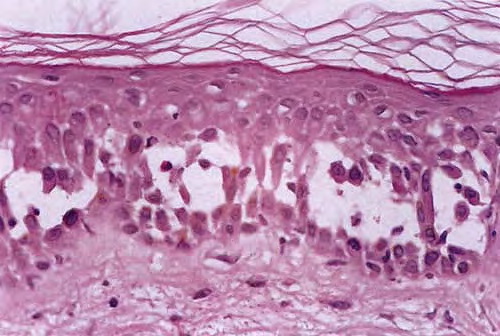
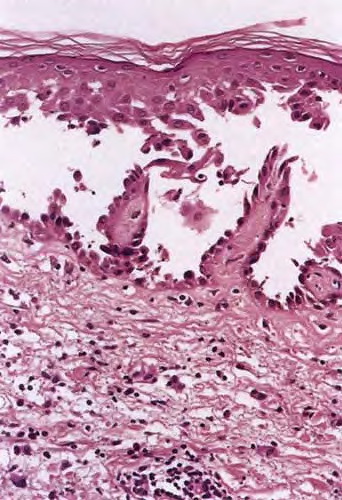
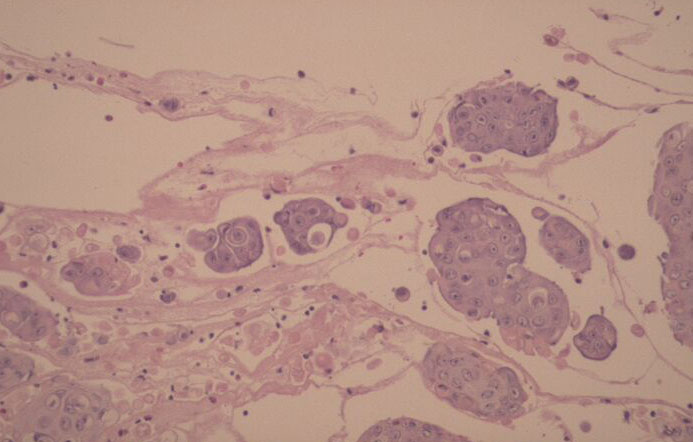
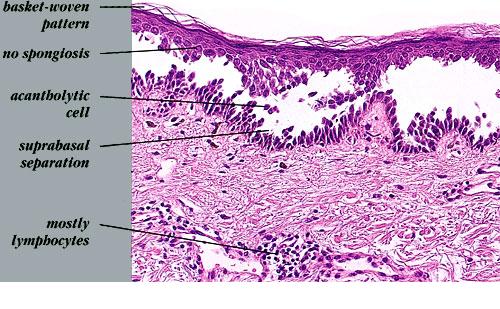
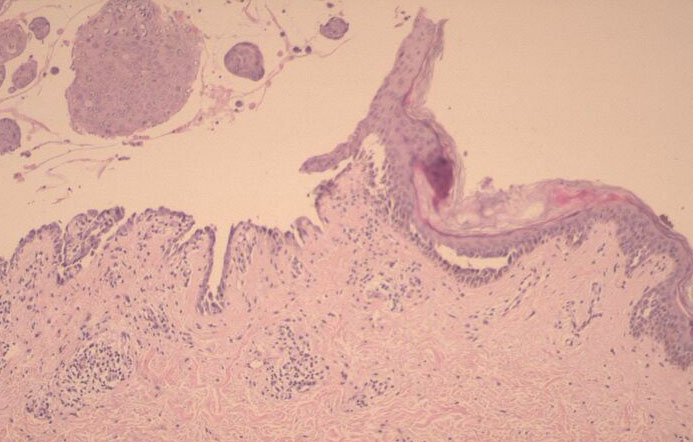
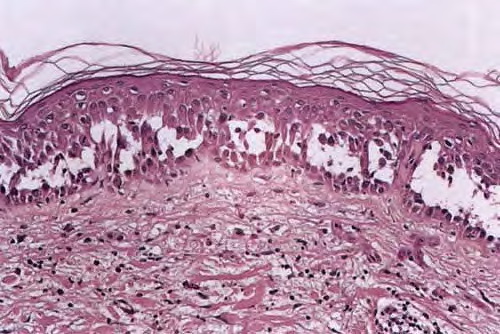
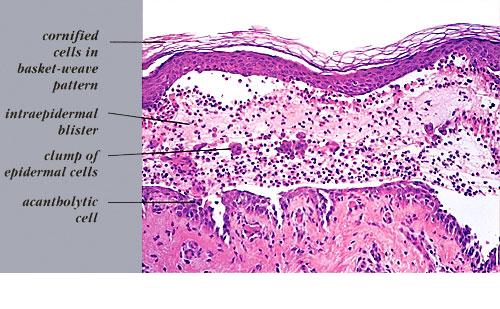
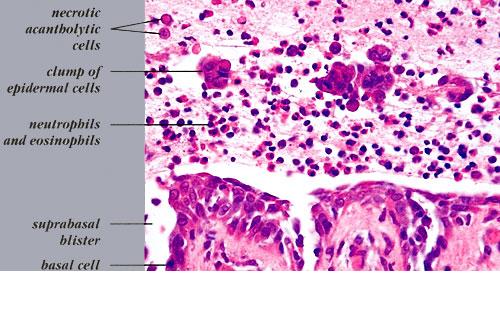
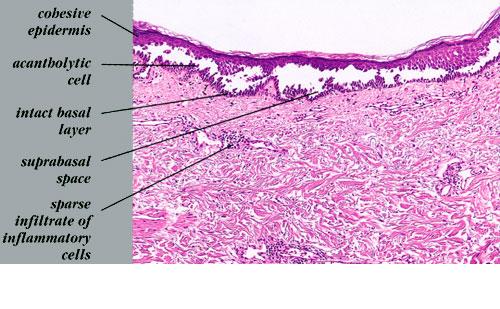
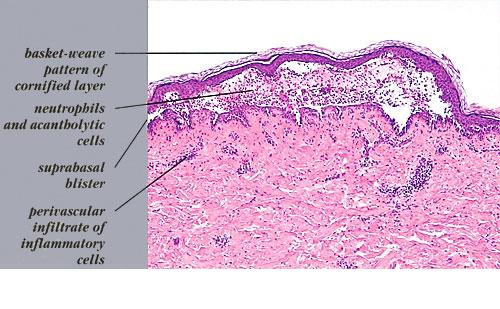
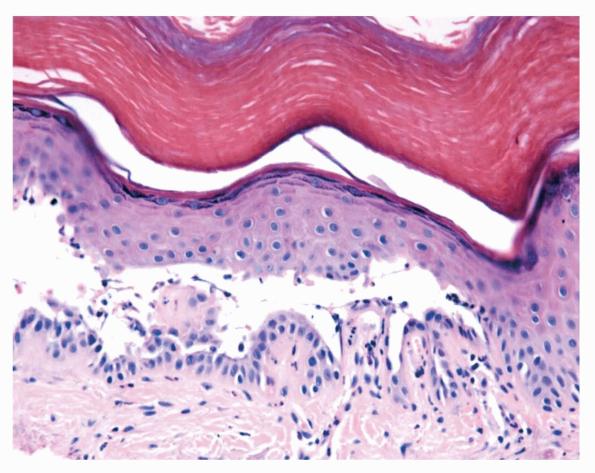
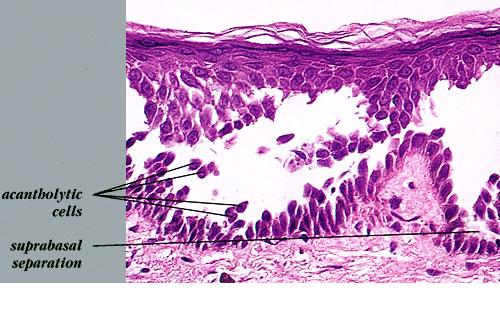
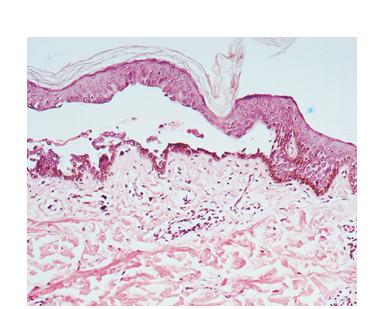
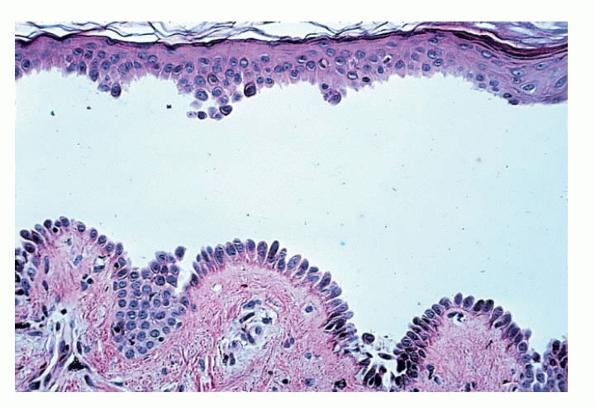
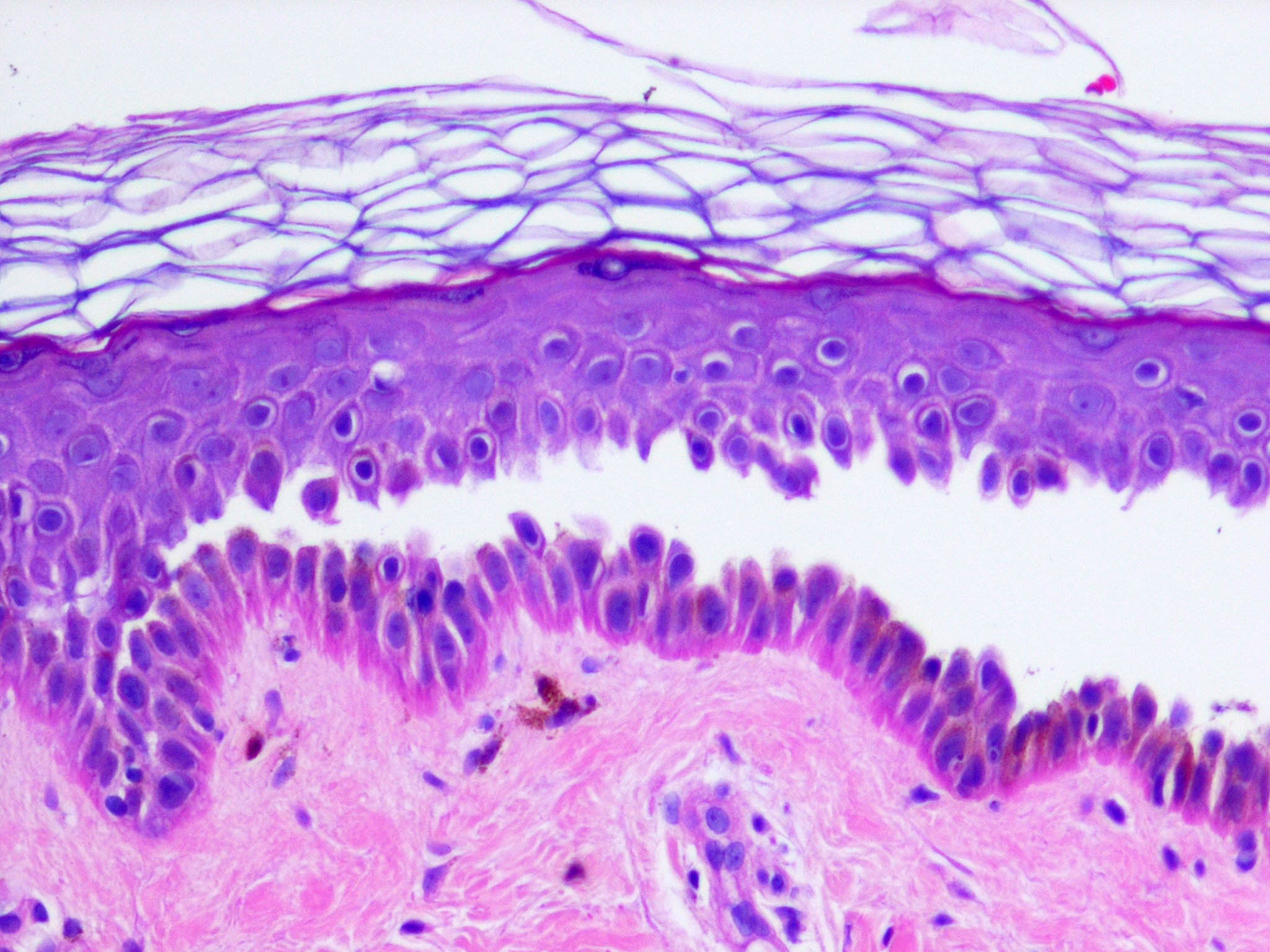
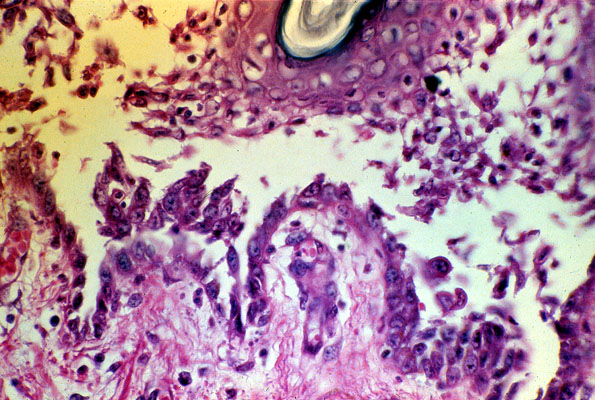
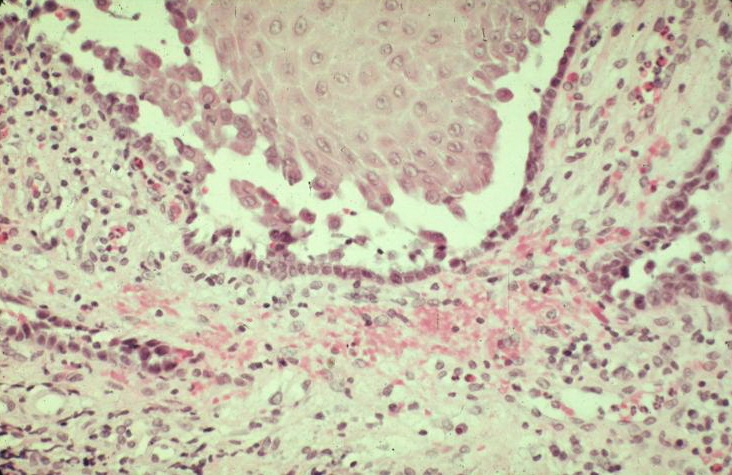
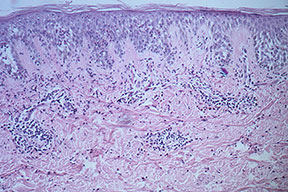
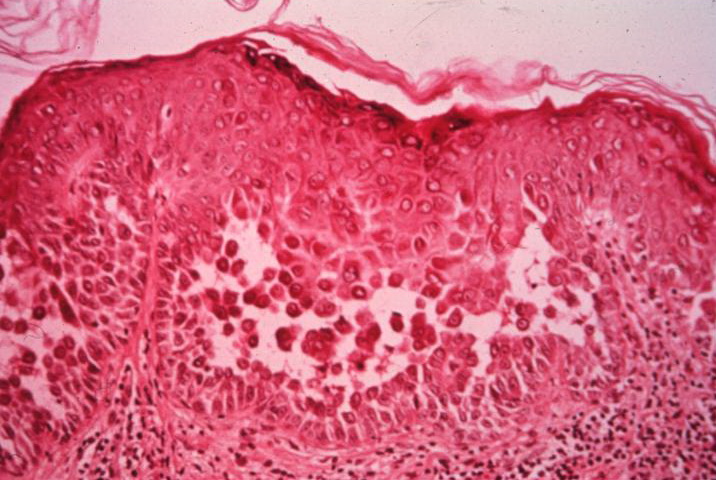
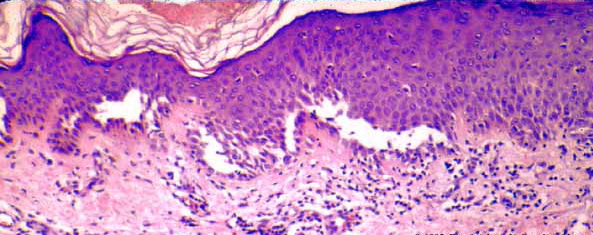
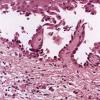
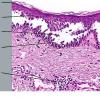
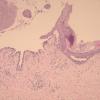
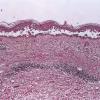
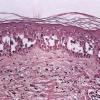
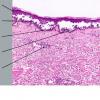
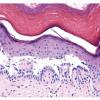
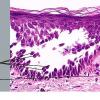
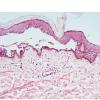
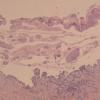
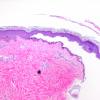
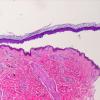
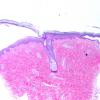
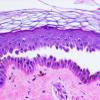
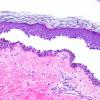
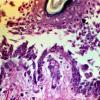
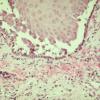
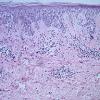
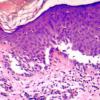
The earliest recognized change may be either eosinophilic spongiosis rarely or, more commonly, "spongiosis" in the lower epidermis . This spongiosis may actually represent the earliest manifestation of acantholysis rather than true spongiosis as defined earlier. Acantholysis leads first to the formation of clefts and then to blisters in a predominantly suprabasallocation . The intraepithelial acantholysis may extend into adnexal structures or occasionally be higher in the stratum spinosum. The basal keratinocytes, although separated from one another through the loss of attachment, remain firmly attached to the dermis like a "row of tombstones." Within the blister cavity, the acantholytic keratinocytes, singularly or in clusters, have rounded condensed cytoplasm about an enlarged nucleus with peripherally palisaded chromatin and enlarged nucleoli. In some patients, there are varying quantities of antidesmoglein 1 and antidesmoglein 3 antibodies, leading to variable planes of acantholysis. There is little inflammation in the early phase of blister formation. If present, it is usually a sparse, lymphocytic perivascular infiltrate accompanied by dermal edema. However, if eosinophilic spongiosis is apparent, numerous eosinophils may infiltrate the dermis. The phenomenon of eosinophilic spongiosis occurs occasionally in other blistering diseases, particularly in their early phases, including acute contact dermatitis, pemphigus foliaceus, bullous pemphigoid, herpes gestation is, drug eruptions, spongiotic arthropod bite reactions, and transient acantholytic dermatosis. Several important changes ensue as the lesions age. First, a mixed inflammatory cell reaction consisting of neutrophils, lymphocytes, macrophages, and eosinophils may develop. Because of the instability of the blister roof, erosion and ulceration may occur. Older blisters may also have several layers of keratinocytes at the blister base because of keratinocyte migration and proliferation. Last, there may be considerable downward growth of epidermal strands, giving rise to so-called villi (Fig. 9-9D). The evaluation of patients with only oral lesions is difficult, because intact blisters are rarely encountered due to the trauma of mastication, and biopsies may show only erosion and ulceration. Indeed, it is best to sample the edge of a denuded area with intact mucosa in an attempt to demonstrate the typical pathologic changes. Clinicians frequently cannot distinguish between an ulcer and the intact mucosa, as both are often white and shaggy. In patients with only oral lesions, biopsies of intact oral mucosa for DIF testing are more sensitive than biopsies of lesions for routine light microscopic evaluation. Therefore, biopsy from the normal maxillary and upper buccal mucosa is necessary when there is extensive ulceration. Cytologic examination using a Tzanck preparation is useful for the rapid demonstration of acantholytic epidermal keratinocytes in the blisters of pemphigus vulgaris. For this
purpose, a smear is taken from the underside of the roof and from the base of an early, freshly opened bulla. Giemsa stain is applied with subsequent rinsing and air-drying.
|
|
Because acantholytic keratinocytes are occasionally seen in various nonacantholytic vesiculobullous or pustular diseases as a result of secondary acantholysis, cytologic examination represents merely a preliminary test and should not supplant histologic examination.
|
|
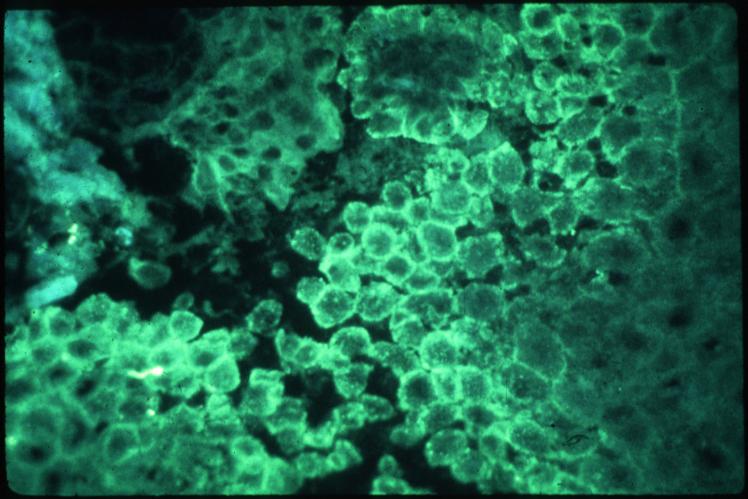
Immunofluorescence (IF) Testing.
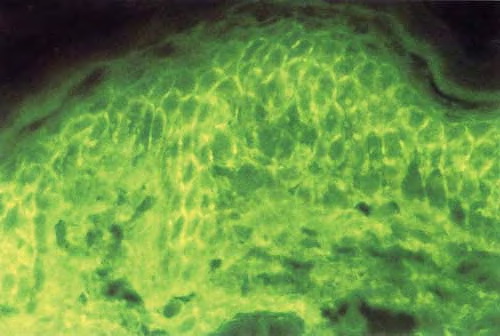
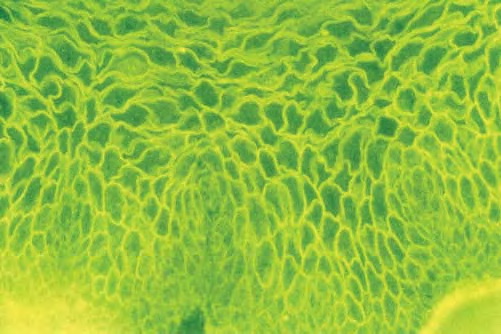
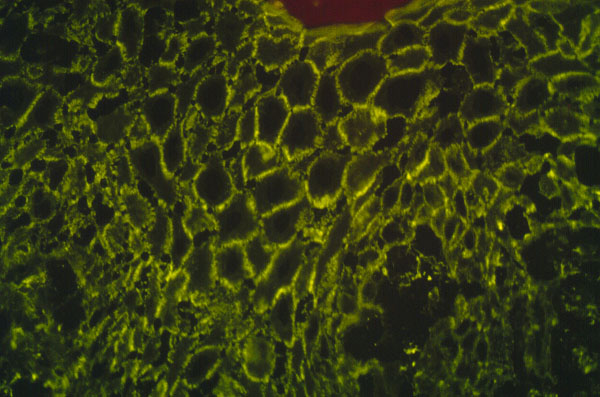
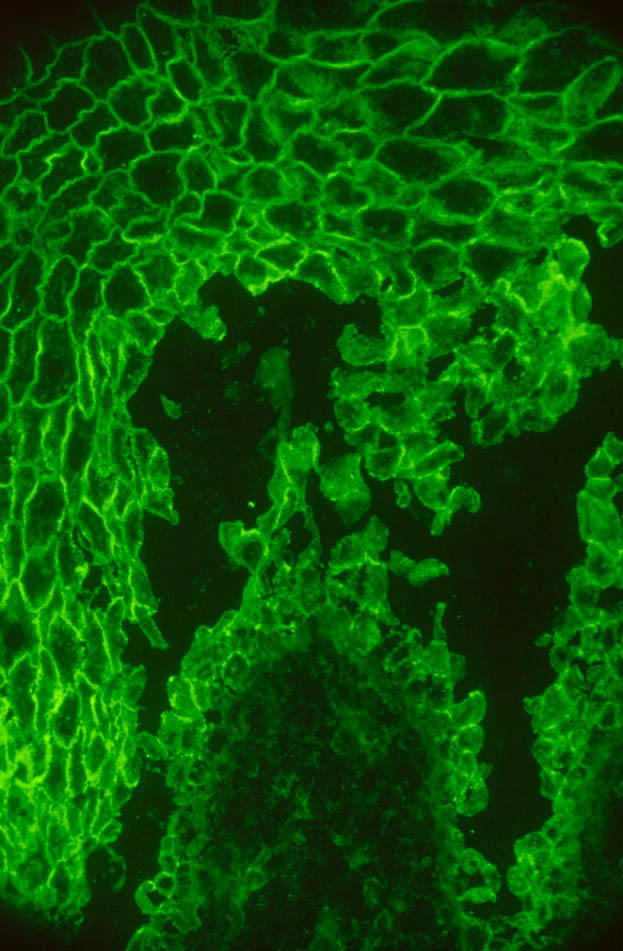
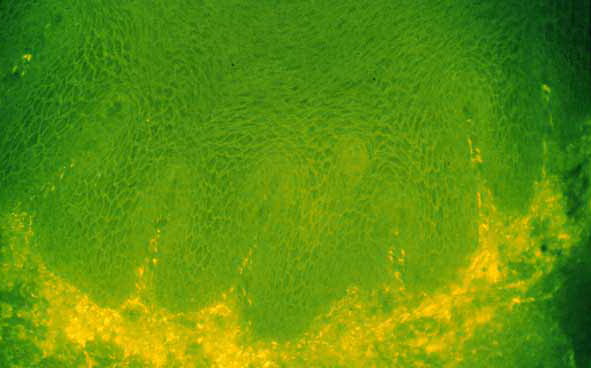
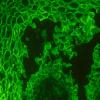
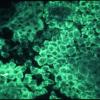
The edge of a blister with intact surrounding normal skin, uninvolved skin adjacent to a blister, or adjacent erythematous skin should be supplied for study. The tissue may be snap-frozen or transported in Michel's medium. DIF testing is a very reliable and sensitive diagnostic test for pemphigus vulgaris, in that it demonstrates lacelike IgG in the squamous intercellularlcell surface areas in up to 95% of cases, including early cases and those with very few lesions, and in up to 100% of cases with active disease . It remains positive, often for many years after clinical disease has subsided. In late lesions, when acantholysis is well developed, the lacelike intercellularlcell surface pattern of IgG may become dotlike, paralleling electron microscopic findings and correlating with aggregation of desmosomes on the cell surface. Negative DIF findings when the patient is in
remission may be a good prognostic indicator . At this time, DIF testing is incorrectly thought by most to be free
of false positives; however, false positives may occur. On occasion, it may be difficult to distinguish intercellular
staining of pemphigus from nonspecific staining; for example, spongiotic dermatitis, psoriasis, bullous impetigo,
and epidermis adjacent to ulcers secondary to a number of disorders may have squamous intercellular substance
IgG due to the presence of serum in the intercellular substance. Often, IgM, IgA, fibrinogen, and albumin are
present as well, indicating nonspecific trapping in the false-positive tests. lmmunoperoxidase methods have
achieved roughly the same sensitivity as the IF method, but they have not replaced IF testing as the prime
diagnostic tool. For IIF testing, unfixed frozen sections of guinea pig esophagus, monkey esophagus, or normal
human skin are used as substrate. In general, monkey esophagus is the best substrate for IIF tests. Circulating
IgG autoantibody is demonstrated in the squamous intercellular substance in 80% to 90% of cases , and the
titer correlates with disease activity. False-positive IIF tests occur. In a series of 1,500 patients with circulating pemphigus antibodies, approximately 1 % had no evidence of clinical disease. Antibodies that mimic or may give in
vitro deposition in stratified squamous epithelium in the absence of pemphigus have been reported in burns,
penicillin allergy, toxic epidermal necrolysis (TEN), systemic lupus erythematosus (SLE), myasthenia gravis,
bullous pemphigoid, cicatricial pemphigoid, and lichen planus and in patients with antibodies directed against
blood groups A and B. Such antibodies are present in low titer and are thought to be nonpathogenic.
Antidesmoglein autoantibodies are sometimes found in patients with no bullous disease. For example, they have
been found in patients with silicosis and in relatives of patients with pemphigus vulgaris .
|
|
Pathogenesis. Compelling evidence has accumulated that IgG autoantibodies against desmoglein 3 and desmoglein 1 are pathogenic and playa primary role in inducing the blister formation in pemphigus. Affinitypurified IgG from pemphigus vulgaris sera recognizes the extracellular domain of desmoglein 3 and causes suprabasal acantholysis when injected into neonatal mice . Furthermore, when antidesmoglein 3 IgG from pemphigus vulgaris is immunoabsorbed with the extracellular domains of desmoglein 3, those sera no longer have the ability to cause blisters in neonatal mice . Although the pathogenic role of antidesmoglein 3 autoantibodies in blister formation is assured, the exact sequence of events that occur after antibody binding is not totally understood. Conformational epitope mapping of desmoglein 3 in pemphigus vulgaris suggests that the amino terminal residue 1-161 is the target of autoantibodies . This segment is in the extracellular domain that is essential for cell-cell adhesion. One possibility is that these antibodies interfere directly with the adhesive interaction of desmogleins between cells by steric hindrance. Another possibility is that the disruption of cell-cell adhesion is mediated by signal transduction. Proteinases, likely induced by pemphigus antigen-antibody union,
are thought to play an important role in acantholysis. Although complement fixation by pemphigus antibodies may
|
|
promote acantholysis, acantholysis occurs in experimental systems in the absence of complement. The stimulus for the formation of autoantibodies is unknown, although drugs, viral infection, trauma, ionizing radiation, and PUVA therapy have been implicated because they have preceded the onset of pemphigus. Pemphigus vulgaris is rarely associated with internal cancer, Castleman's disease, thymoma, myasthenia gravis, localized scleroderma, Grave's disease, and SLE.
|
|
Ultrastructural Study. The intercellular cement substance, or glycocalyx, is partially or entirely lysed in lesions with early acantholysis. There is widening of the intercellular spaces with intact desmosomes. As the intercellular space is widened, there is separation of the two opposing attachment plaques of the desmosomes; thus, single attachment plaques, with adherent tonofilaments, are seen at the periphery of keratinocytes. As acantholysis progresses, the desmosomes gradually disappear and the keratinocytes develop numerous cytoplasmic
processes that often interdigitate with one another. All of the early ultrastructural changes in pemphigus vulgaris are extracellular. Only subsequent to the dissolution of the desmosomes does retraction of the tonofilaments to the perinuclear area develop with ultimate degeneration of the acantholytic cells. The cohesion of the basal keratinocytes with the basement membrane zone is not affected in pemphigus vulgaris because of the preservation of structures connecting the basal keratinocytes with the dermis. Immunoelectron microscopy shows that the immunoglobulins are deposited on the surface of the keratinocytes in a discontinuous globular pattern in the extracellular domains of desmosomes .
|
|
Differential Diagnosis. In early blisters that are free of secondary changes, such as the degeneration or regeneration of epidermal cells, the histopathology of pemphigus vulgaris is characteristic. Important differential diagnoses include Hailey-Hailey disease and transient acantholytic dermatosis. Hailey-Hailey disease has fullthickness ("dilapidated brick wall") acantholysis, epidermal hyperplasia, and an impetiginized scale crust. The acantholysis does not extend down follicles as it does in pemphigus. Transient acantholytic dermatosis may exhibit small foci of intraepidermal acantholysis, but these are only a few rete wide in contrast to the uniform widespread acantholysis observed in biopsies of pemphigus vulgaris. Disorders such as Darier's disease that are characterized by acantholytic dyskeratosis are readily separated from pemphigus vulgaris by the presence of abnormal granular keratinocytes and parakeratotic cells, so-called corps ronds and corps grains. Although light microscopic examination of pemphigus lesions is important, positive DIF is the gold standard in diagnosis at this time and must be pursued in all cases in which pemphigus vulgaris is considered.
|
|