|
Necrobiois lipoidica diabeticorum = النخر الشحماني السكري |
 |
 |
 |
|
Necrobiosis Lipoidica
Necrobiosis lipoidica is an idiopathic disorder typified by indurated plaques of the shins . In 1966, in a large series, Muller and Winkelman reported that two thirds of patients with necrobiosis lipoidica had overt diabetes at the time of diagnosis {82}. Of the rest, all but 10% developed diabetes within 5 years, had abnormal glucose tolerance, or had a history of diabetes in at least one parent . In a more recent series, only 11 % of patients had diabetes at presentation, with an additional 11 % developing diabetes or impaired glucose tolerance over 15 years . Of all patients with diabetes, fewer than 1 % develop necrobiosis lipoidica . Some reports have suggested that necrobiosis lipoidica heralds more rapid progression of diabetes in patients with that disorder .
|
|
In well-developed necrobiosis lipoidica, one observes one or several sharply but irregularly demarcated patches or plaques, usually on the shins . Usually they are bilateral, and the condition is more often present in women . The lesions appear yellow-brown in the center and purplish at the periphery. Whereas the periphery of the lesions may show slight induration, the center of the lesions gradually becomes atrophic, shows telangiectases, and may ulcerate. When lesions first begin, red-brown papules can be observed. In addition to the shins, lesions may be present elsewhere on the lower
|
|
extremities, including the ankles, calves, thighs, popliteal areas, and feet. In about 15% of the cases, lesions are present also in areas other than the legs, especially on the dorsa of the hands, fingers, and forearms. Rarely, the head and abdomen are affected. Necrobiosis lipoidica with lesions exclusively outside the legs is extremely rare; it is reported to occur in 1 % of patients with necrobiosis lipoidica .
|
|
Lesions located in areas other than the legs may appear raised and firm and may have a papular, nodular, or plaquelike appearance without atrophy. Clinically they may resemble granuloma annulare . Involvement of the scalp by large, atrophic patches occurs occasionally. This is usually seen in association with lesions on the shins and elsewhere but also, rarely, in isolation .
|
|
In rare instances, transfollicular elimination of necrotic material takes place in necrobiosis lipoidica, producing small hyperkeratotic plugs within a plaque . Necrobiosis lipoidica occasionally coexists with sarcoid or granuloma annulare . Rare examples of squamous cell carcinoma arising in lesions of necrobiosis lipoidica have been reported .
|
|
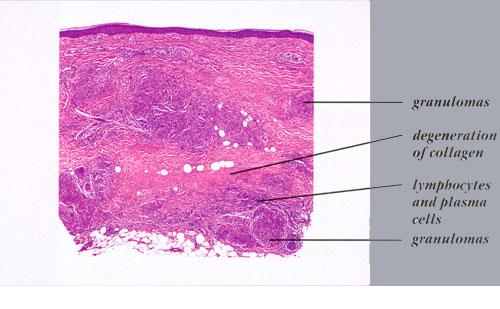
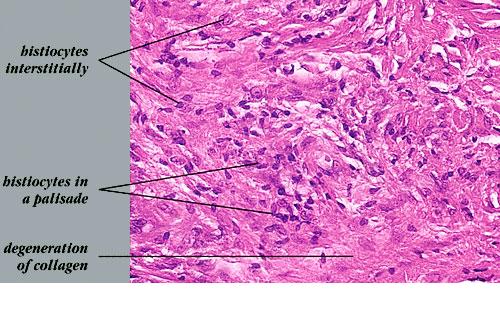
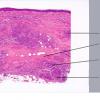
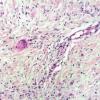
Histopathology.
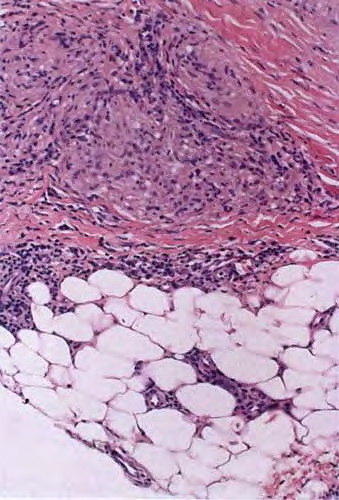
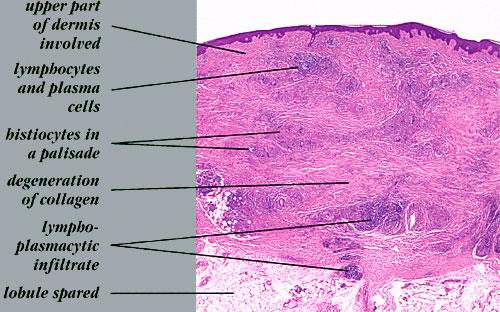
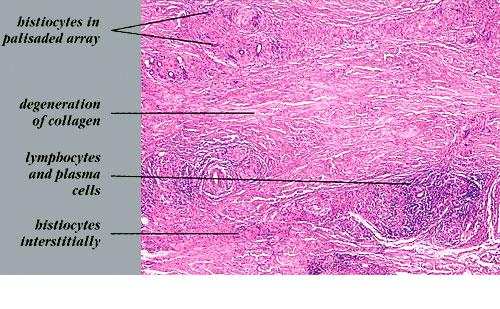
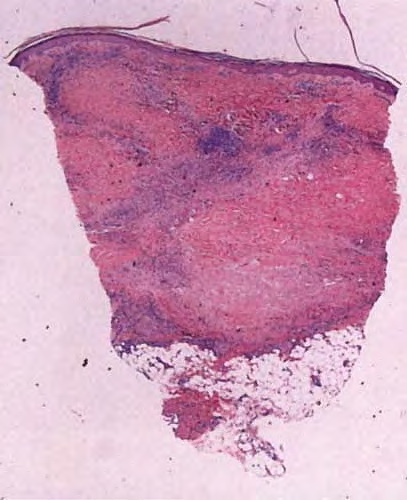
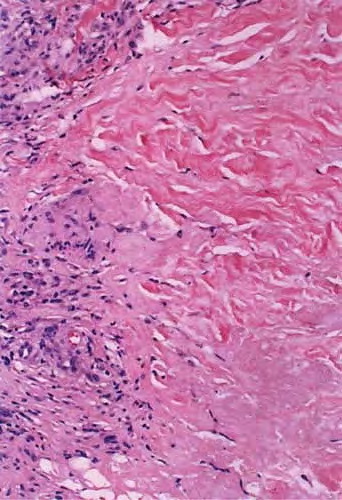
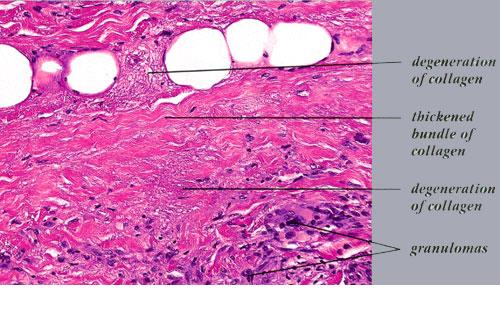
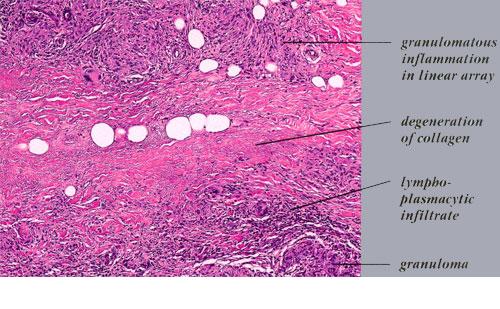
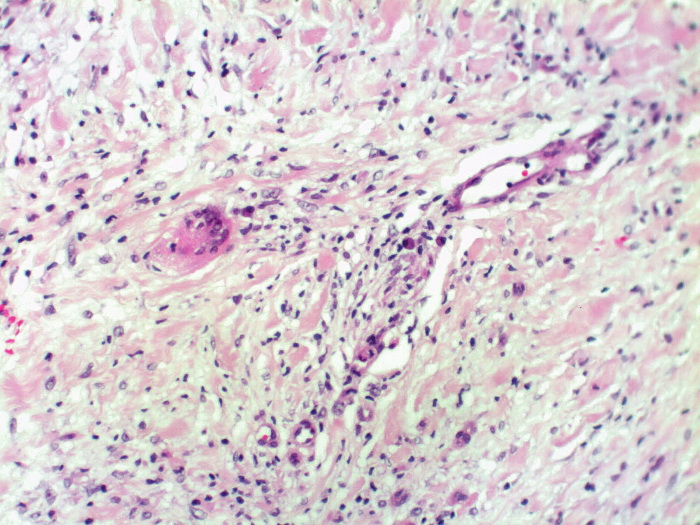
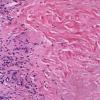
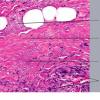
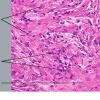
On histologic examination, the epidermis may be normal, atrophic, or hyperkeratotic. In some instances, the surface of the biopsy shows ulceration. Usually the entire thickness of the dermis or its lower two thirds is affected by a process that exhibits a variable degree of granulomatous inflammation, degeneration of collagen, and sclerosis . Histologic changes of necrobiosis lipoidica may be seen in subcutaneous septae . Occasionally only the upper dermis is affected . The granulomatous component is usually conspicuous, and the histiocytes mayor may not be arranged in a palisade. Occasionally there are just a few scattered epithelioid histiocytes and giant cells. The latter picture is more likely to occur in sections in which sclerosis is extensive, and occasionally in such biopsies several sections must be examined before a granulomatous component becomes apparent. Giant cells are usually of the Langhans or foreign-body type; occasionally, Touton cells or asteroid bodies are seen. If the histiocytes are arranged in a palisade, the palisades tend to be somewhat horizontally oriented andlor vaguely tiered. Occasionally, histiocytes may be seen completely to encircle altered connective tissue, particularly degenerated collagen, but, more commonly, altered connective tissue is incompletely surrounded by histiocytes. This alteration of connective tissue has also been referred to as "necrobiosis." The altered collagen appears different from normal collagen by having a paler, grayer hue and by appearing more fragmented and haphazardly arranged; it may also appear more compact or smudged . Areas of sclerosis with a diminished number of fibroblasts can be seen. A clue to the presence of sclerosis can be found by looking at the edges of the biopsy specimen, which tend to be straight with less of the inward retraction of the dermis ordinarily associated with punch biopsies . Increased mucin is usually inapparent or subtle in contrast to granuloma annulare. Other findings include a sparse to moderately dense, primarily perivascular lymphocytic infiltrate, plasma cells in the deep dermis in some biopsies , involvement of the upper subcutis with thickened fibrous septa, and lipids which may be present in foamy histiocytes , which may be inferred from the presence of cholesterol clefts or can be detected extracellularly with special stains on fresh tissue. Cholesterol clefts are rare, seen in less than 1 % of cases . Deep lymphoid follicles may be present in up to 10% of cases . Older lesions show telangiectases superficially. Blood vessels, particularly in the middle and lower dermis, often exhibit thickening of their walls with proliferation of their endothelial cells. The process may lead to partial and rarely to complete occlusion of the lumen. The thickened walls may be infiltrated with periodic acid-Schiff (PAS)-positive, diastase-resistant material . Vascular changes of this type are seen particularly near foci containing thickened, hyalinized collagen
|
|
bundles. Whereas the vascular changes often are conspicuous in lesions of the lower legs, they usually are mild or absent elsewhere . Histologic findings that are possibly correlated with the clinical presence of diabetes include florid palisading around degeneration of collagen and cholesterol clefts .
|
|
Pathogenesis. The cause of necrobiosis lipoidica is unknown, and it is unclear whether the degeneration of collagen is a primary or a secondary event . Some authors have postulated that the degeneration of collagen is the result of vascular changes secondary to clinical or latent diabetes . However, evidence against a vascular cause includes the absence of vascular pathology in approximately one third of biopsies examined and the fact that vessels that are affected are often situated in the lower dermis and are of a larger caliber than the vessels affected by diabetic microangiopathy. Abnormal glucose transport by fibroblasts has also been implicated .
|
|
Electron microscopic examination shows degenerative changes in collagen and elastin with loss of cross-striation in collagen fibrils. Collagen synthesis by fibroblasts is diminished .
|
|
Direct immunofluorescence studies have shown that necrobiotic foci contain fibrinogen. Deposits of immunoglobulin and C3 have been found in the vessel walls , but this is not a consistent finding .
|
|
Differential Diagnosis. Differentiation of necrobiosis lipoi-dica from granuloma annulare was discussed in the
|
|
section on granuloma annulare.
|
|
Occasionally, necrobiosis lipoidica shows discrete collections of epithelioid cells that may resemble those seen in sarcoidosis . However, significant alteration of the collagen is usually present in necrobiosis lipoidica and absent in sarcoidosis .
|
|
Necrobiotic xanthogranuloma with paraproteinemia can simulate necrobiosis lipoidica but differs by showing a denser, more diffuse infiltrate with a greater number of foamy histiocytes, Touton giant cells, more extensive inflammation of the subcutis, and greater disruption of normal subcutaneous architecture. Lymphoid follicles and cholesterol clefts are more commonly seen in necrobiotic xanthogranuloma than in necrobiosis lipoidica .
|
|
Differentiation of necrobiosis lipoidica from annular elastolytic granuloma was discussed in the section on annular elastolytic granuloma.
|
|
|
|
|