|
Morphea
In morphea, or circumscribed scleroderma, the lesions usually are limited to the skin and to the subcutaneous tissue beneath the cutaneous lesions. Occasionally, however, the underlying muscles and rarely the underlying bones are also affected.
|
|
Morphea may be divided according to morphology and distribution of lesions into six types: guttate, plaque, linear, segmental, subcutaneous, and generalized. Eosinophilic fasciitis, even though it is the fascial component of subcutaneous morphea, is discussed separately because of its somewhat different clinical and histologic appearance.
|
|
Guttate lesions occur almost always in association with lesions of the plaque type. Guttate lesions are small and superficial; they resemble the lesions of lichen sclerosus et atrophicus but do not show hyperkeratosis or follicular plugging.
|
|
Lesions of the plaque type-the most common manifestation of morphea-are round or oval but through coalescence may assume an irregular configuration. They are indurated, have a smooth surface, and show an ivory color. As long as they are enlarging, they may show a violaceous border, the so-called lilac ring.
|
|
Lesions of the linear type occur predominantly on the extremities and on the anterior scalp. When one or several extremities are involved, there is often, in addition to induration of the skin, marked atrophy of the subcutaneous fat and of the muscles, resulting in contractures of muscles and tendons and ankyloses of joints. In children it may result in impaired growth of the affected limb . On the anterior portion of the scalp and on the forehead, linear morphea often has the configuration of the stroke of a saber (coup de sabre) .
|
|
Segmental morphea occurs on one side of the face, resulting in hemiatrophy. Occasionally, morphea en coup de sabre and facial hemiatrophy occur together (98). This manifestation of morphea typically occurs in children and can often be associated with neurologic deficits . Due to a high incidence of overlap between the two conditions and the similar histopathology, some authors feel that they represent slightly different manifestations of the same process. Retrospective studies have estimated the coincidence of the conditions at between 36% and 42% .
|
|
In subcutaneous morphea (morphea profunda) the involved skin feels thickened and bound to the underlying fascia and muscle. The involved plaques are ill defined, and the skin of these plaques is smooth and shiny .
|
|
Generalized morphea comprises very extensive cases showing a combination of several of the five types just described. Although it is seen mainly in children, in whom it has been described as disabling pansclerotic morphea , it
|
|
can also occur in adults. Rarely, bullous lesions are seen in patients with generalized morphea .
|
|
There are several reported cases of morphea that involve the superficial reticular dermis (superficial morphea) as contrasted with its usual involvement of the deep reticular dermis . The clinical impact of the depth of involvement is unclear. The coexistence of lesions of morphea and lichen sclerosus et atrophicus is worthy of note.
|
|
There is conflicting data regarding Borrelia burgdorferi infection in cases of morphea. Studies indicating that such
|
|
a relationship exists are primarily from Europe . Studies in North America and some from Europe have resulted in negative findings .
|
|
Histopathology.
The different types of morphea cannot be differentiated histologically. Rather, they differ in regard to severity and depth of involvement of the skin. Therefore, it is of great importance that the biopsy specimen include adequate subcutaneous tissue because most of the diagnostic alterations are seen in the lower dermis and in the subcutis.
|
|
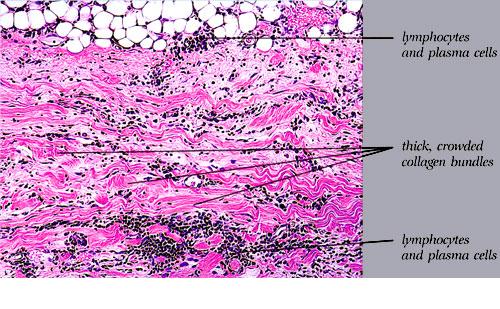
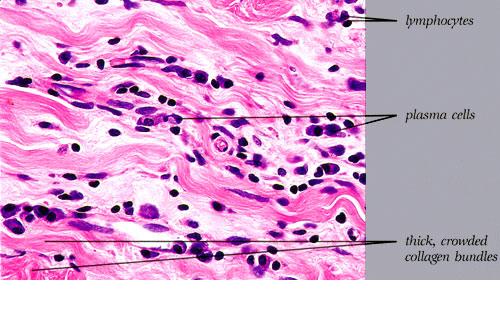
Early inflammatory, intermediate, and late sclerotic stages exist. In the early inflammatory stage, found particularly at the violaceous border of enlarging lesions, the reticular dermis shows interstitial Iymphoplasmacytic infiltrates with or without eosinophils among slightly thickened collagen bundles . As lesions become established, the inflammatory infiltrates surround eccrine coils and are associated with hypocellular collagen bundles and reduced numbers of surrounding adipocytes . A much more pronounced inflammatory infiltrate than that seen in the dermis often involves the subcutaneous fat and extends upward toward the eccrine glands. Trabeculae subdividing the subcutaneous fat are thickened because of the presence of an inflammatory infiltrate and deposition of new collagen. Large areas of subcutaneous fat are replaced by newly formed collagen, which is composed of fine, wavy fibers rather than bundles and stains only faintly with hematoxylin-eosin . Vascular changes in the early inflammatory stage generally are mild both in the dermis and in the subcutaneous tissue. They may consist of endothelial swelling and edema of the walls of the vessels (1 OB).
|
|
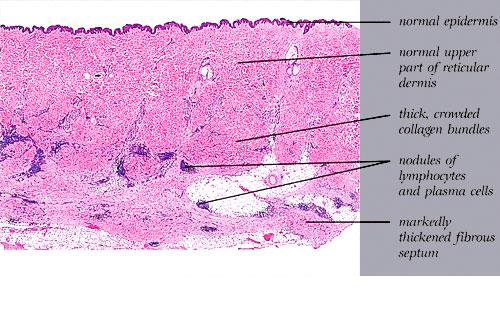
In the late sclerotic stage, as seen in the center of old lesions, the inflammatory infiltrate has disappeared almost completely, except in some areas of the subcutis. The epidermis is normal. The collagen bundles in the reticular dermis often appear thickened, closely packed, and hypocellular and stain more deeply eosinophilic than in normal skin (Fig. 10-13C, D). In the papillary dermis, where the collagen normally consists of loosely arranged fibers, the collagen may appear homogeneous.
|
|
The eccrine glands appear markedly atrophic, have few or no adipocytes surrounding them, and appear surrounded by newly formed collagen . In addition, instead of lying near the dermal-subcutaneous junction as in normal skin, they seem to lie higher in the dermis as a result of the replacement of most of the subcutaneous fat by newly formed collagen. This collagen consists of thick, pale, sclerotic, homogeneous, or hyalinized bundles with only few fibroblasts (hypocellular). Few blood vessels are seen within the sclerotic collagen; they often have a fibrotic wall and a narrowed lumen. Elastic stains show thick elastic
fibers arranged parallel to hypocellular collagen strands and parallel to the epidermal surface .
|
|
The fascia and striated muscles underlying lesions of morphea may be affected in the linear, segmental,
|
Subcutaneous , and generalized types. The fascia shows fibrosis and sclerosis similar to that seen in subcutaneous tissue. The muscle fibers appear vacuolated and separated from one another by edema and focal collections of inflammatory cells
|
Bullae, seen only on rare occasions in generalized and in subcutaneous morphea, arise subepidermally, probably as a result of lymphatic obstruction, causing subepidermal edema.
|
|
Differential Diagnosis. Contrasting features of morphea and lichen sclerosus et atrophicus are summarized in. They include relatively little epidermal change in morphea, as compared with thinning of the rete ridges, follicular plugging, and interface alterations of lichen sclerosus. The reticular dermal changes of fibrosis and inflammation in morphea contrast with the edema and loss of elastic tissue in lichen sclerosus. Histologic differentiation of the late stage of morphea from lichen sclerosus et atrophicus may cause difficulties, particularly in view of the fact that the two conditions may coexist.
|
|