|
Malignant Melanoma
Most malignant melanomas arise in the epidermis and these may be in situ (entirely within the epidermis) or invasive (extending from the epidermis into the dermis). Occasional invasive melanomas are entirely dermal at presentation. Invasive melanoma may be tumorigenic ("vertical growth phase") or non tumorigenic ("radial growth phase"). Melanoma in situ and nontumorigenic invasive melanoma can be divided into (a) lentigo maligna, (b) superficial spreading, (c) acral-Ientiginous, and (d) mucosallentiginous types. Tumorigenic melanoma may arise in relation to a preexisting nontumorigenic component of any of the foregoing types, in which case it is named accordingly. Alternatively, tumorigenic melanoma may arise de novo, without evidence of an adjacent in situ or microinvasive component at the time of detection, in which case it is termed (e) "nodular melanoma." However, some but all of these lesions probably arise initially via a nontumorigenic intraepidermal component that fails to develop or persist as the tumorigenic component evolves. Important variants of tumorigenic melanoma include (f) desmoplastic melanoma and (g) neurotropic melanoma. Other unusual forms of tumorigenic melanoma are discussed later.
|
|
All major types of melanoma originate almost invariably from melanocytes at the epidermal-dermal junction. Although the lesions are commonly associated with a preexisting nevus,
|
|
more than half of them arise either de novo or have completely supplanted the precursor nevus at the time of presentation. The majority of cutaneous melanomas are believed to be caused by sunlight exposure, either intermittent (sunburn episodes) in the more common superficial spreading melanomas or chronic in the lentigo maligna melanomas. The cause of acral and mucosal melanomas is unknown.
|
|
Classification of Melanoma
|
|
There are two major categories of melanoma, which represent sequential stages or phases of stepwise tumor progression . In the nontumorigenic radial or horizontal growth phase, the neoplastic melanocytes (melanoma cells) are confined to the epidermis (melanoma in situ) or to the epidermis and papillary dermis without evidence of proliferation in the dermis and without formation of an expansile tumor mass. These lesions may be confined to the epidermis (in situ melanoma), or there may be a few cells in the dermis (microinvasive melanoma). This phase may be followed after varying lengths of time by the focal appearance of the mitogenic and/or tumorigenic vertical growth phase, or a phase of dermal invasion with capacity for not only cell survival, but also proliferation in the dermis and usually with expansile tumor formation. Thus, a fully evolved melanoma may have two major lesional compartments: the nontumorigenic, in situ or microinvasive radial growth phase, placed within which there may be a contiguous tumorigenic vertical-growth-phase compartment. In addition, dermal and/or epidermal compartments of an associated nevus may be recognized in some melanomas.
|
|
About 5% to 10% of melanomas in different series fall into "unclassified" or "other" categories . The fact that categorization of an individual case is occasionally difficult does not mean that classification of melanoma, after accounting for tumor thickness and site, is unnecessary, as has been stated . Even though in the tumorigenic stage the prognosis is similar for all four types of melanoma, depending largely on the depth of invasion, the duration of the in situ phase preceding lentigo maligna melanoma is, on the average, longer than that of superficial spreading melanoma . Furthermore, there are differences in the apparent etiology of the various forms of melanoma and in their molecular biology In a recent important study, attributes traditionally used in the classification of melanomas into the aforementioned clinicopathologic subtypes correlated strongly with the mutation status of the tumors studied. An algorithm involving an initial separation based on melanoma cell nesting and scatter, followed by consideration of cell size and age, predicted BRAF mutation with an error estimate of 13%, demonstrating that parameters routinely available and traditionally used by practicing pathologists allow good prediction of BRAF mutation status. It was concluded that this "strong association between genetic alterations and morphological findings further supports the existence of biologically distinct melanoma types, and the use of genetic factors to develop and clarify improved clinically applicable classification systems" .
Finally, the separate description of the morphologic variants has nosologic and pedagogic value, facilitating accurate diagnosis by enabling the recognition of the variant patterns.
|
|
Morphology of Tumorigenic and Nontumorigenic Melanoma
In their nontumorigenic stage, melanomas tend to expand more or less inexorably along the radii of an imperfect circle as viewed clinically. The clinically derived term "radial" growth has no intuitive histologic meaning, and the histologic term "horizontal growth phase" has been suggested as an alternative. The major clinical diagnostic criteria have been summarized as the ABeD criteria (, which include lesional asymmetry (one half of a lesion does not match the other in shape or in color distribution), lesional border irregularity (lesions tend to have an indented coastline like the map of a small island), lesional color variegation (the surface is multicolored and may include shades of tan, brown, blue-black, gray-white, and other variations), and lesional diameter generally greater than 6 mm (although some melanomas are smaller) . These criteria, although useful, are imperfect;
|
|
recent guidelines have emphasized the value of the "ugly duckling" sign of the changing or different-looking mole in the practice of skin self-examination . In view of this, the letter E could be added to the criteria to indicate the "evolving" nature of a changing melanocytic lesion.
|
|
Histologically, most of the lesional cells in nontumorigenic melanomas are located in the epidermis. Microinvasion is here defined as the presence of a few lesional cells in the papillary dermis, without tumorigenic proliferation, which is defined later. Microinvasive lesions are not specifically distinguishable from in situ melanomas on clinical grounds. It has been questioned whether microinvasive or in situ, nontumorigenic melanomas lack competence for metastasis; in a database of 624 clinical stage I invasive melanoma cases followed 10 years or more, the 8-year survival rate from 161 microinvasive or in situ (pure radial growth phase) melanomas was 100 ± 1%. In the same database, the patients with lesions having only radial growth phase were 4.3 years younger than those additionally having vertical growth phase, consistent with the hypothesis that the radial growth phase is antecedent and relatively indolent .
|
|
Clinically, the tumorigenic vertical growth phase is qualitatively different from the plaquelike radial growth phase. The tumor appears as an expanding papule within a previously indolent plaque lesion and grows in three dimensions in a balloon-like fashion to form a nodule . Typically, the ABCD criteria do not apply to the tumor nodule itself, which is commonly symmetric with smooth borders. The color is often
|
|
quite uniform and may be pink rather than blue-black, and the diameter of the tumor nodule itself is often less than 6 mm, even in a quite high-risk lesion. For these reasons, clinical diagnosis of melanoma may be subtle in a nodular melanoma that lacks an adjacent nontumorigenic compartment .
|
|
The major histologic feature that distinguishes a tumorigenic melanoma is the capacity for proliferation of melanoma cells in the extracellular matrix of the dermis to form an expansile mass. In contrast, nontumorigenic melanoma cells may proliferate inexorably in the epidermal compartment and may invade the dermis but do not proliferate there . The lack of metastatic capacity in nontumorigenic melanomas may be explained by considering that cell proliferation in the extracellular matrix of a distant site is essential to the development of a metastasis. Thus, it is likely that a tumor that cannot proliferate in the matrix at its local site of origin would not do so in a metastatic site either. Operational definitions for tumorigenic and nontumorigenic melanoma and for radial and vertical growth phase are as follows :
|
|
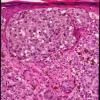
Tumorigenic melanoma. A mass of melanoma cells is present in the dermis, defined as at least one cluster (nest) in the dermis that is larger than the largest intraepidermal cluster (indicative of a tumor with capacity for expansile growth in the dermis) .
|
|
Nontumorigenic melanoma. No mass of melanoma cells is present in the dermis (there is no cluster larger than the largest intraepidermal cluster) .
|
|
Vertical growth phase . A lesion is classified as vertical growth phase if it is tumorigenic or if there are any dermal mitoses even in the absence of architectural criteria for tumorigenic growth. The presence of any mitoses in the dermal component of the melanoma is indicative of a tumor with capacity for expansile growth in the dermis and defines the concept of typical vertical growth phase even in the absence of a frank tumor mass .
|
|
Radial growth phase (RGP). A lesion is classified as radial growth phase only ("pure" RGP, or "radial growth phase confined") if it is nontumorigenic and there are no dermal mitoses. Alternatively, the radial growth phase may be present as a compartment of a complex primary melanoma in which the foregoing histologic criteria apply only to that portion of the melanoma adjacent to the VGP . "Pure" RGP melanoma may be defined as the absence of VGP in a primary melanoma .
|
|
In rare instances, a mass is formed in the dermal component of a melanoma by the accretive piling up of clusters of cells in the absence of any single cluster of cells that is larger than the largest intraepidermal cluster . Reed et al. described these lesions as "variant vertical growth phase" or "accretive vertical growth
phase" . These lesions are nontumorigenic. However, if any mitoses are present in such a lesion, it would meet the criteria for vertical growth phase defined earlier. The prognostic significance of variant vertical growth phase is uncertain. Most examples are thin, with a good prognosis as judged by prognostic models. In our experience, rare instances of metastasis have been associated with the presence of variant vertical growth phase; the overall metastatic rate is exceedingly low, comparable with that associated with other nontumorigenic melanomas.
|
|
In a study conducted by the Pathology Panel of the Cancer Research Campaign in the United Kingdom, the level of agreement for recognition of vertical growth phase was "good" as judged by formal kappa analysis and was improved after discussion of standardized criteria among members of the reviewing panel . Subsequently, two additional studies confirmed this finding .
|
|
Molecular Pathology of Melanoma. Knowledge of the molecular pathology of melanoma has expanded dramatically since the discovery in 2001 of a high frequency of mutation of the oncogene BRAF in primary and metastatic melanomas . In a one study, mutations resulting in the activating V599E amino acid substitution were found in 68% of melanoma metastases, 80% of primary melanomas, and, unexpectedly, 82% of nevi (132). Activating mutations of the oncogene NRAS have also been described in melanomas and in tumor-associated and congenital nevi (133,134, 135). Lesions that have mutated NRAS tend not to have mutated BRAF and vice versa . These data suggest that mutational activation of the RAS/RAF/MAPK mitogenic pathway in nevi is a critical step in the initiation of melanocytic neoplasia but alone is insufficient for melanoma tumorigenesis . The CDKN2A tumor suppressor gene product p16 is highly expressed in nevi , presumably restraining the proliferative pressure in these lesions despite the activating oncogene mutations, in a phenomenon termed "oncogene-induced senescence" . Loss of this suppressor in melanomas, in the context of activated mitogenic signaling pathways, may represent an important mechanism of progression .
|
|
The Nontumorigenic Compartment of Primary Malignant Melanoma (Radial Growth Phase)
The following sections describe the morphology of the nontumorigenic compartments of the different forms of melanoma. Next, we discuss the morphology of the tumorigenic vertical growth phase, which tends to be similar among the different forms. Typically, about 90% of all melanomas have a nontumorigenic compartment, and about half of these also have a tumorigenic focus; about 10% of melanomas, termed nodular melanomas, have a tumorigenic but no in situ or invasive radial-growth-phase compartment.
|
|
Two major patterns of nontumorigenic melanoma can be distinguished: pagetoid and lentiginous. The lentiginous pattern recapitulates the pattern of focally contiguous proliferation of nevus cells in the simplest melanocytic neoplasm, lentigo simplex. However, there is more uniform and complete contiguous basal replacement, and thus the proliferation is continuous, at least in part, between adjacent rete ridges. Pagetoid spread, graphically described as "buckshot scatter" of melanocytes within the epidermis, is the best-known pattern of melanomas. However, many melanomas, including many of the lentiginous ones, are entirely or partly lacking in pagetoid proliferation. In many melanomas, as in nevi, nests of melanocytes are present at the dermal-epidermal junction. These tend to differ from those in nevi in being more variable in size, shape, and orientation and in their more irregular spacing along the junction .
|
|
Not all superficial melanocytic proliferations can be reliably and reproducibly distinguished as either a superficial melanoma or as a nevus. In such cases, we provide a descriptive designation, such as superficial atypical melanocytic proliferation of uncertain significance, with a differential diagnosis. For example, a problematic lesion with dysplastic features and a small focus of pagetoid extension of slightly atypical melanocytes into the epidermis may be signed out as "junctional nevus with severe dysplasia and focal changes suggestive of evolving melanoma in situ." Because the differential diagnosis in these lesions includes melanoma in situ, which could locally persist,
|
|
recur, and grow inexorably, although without metastatic potential at the time of diagnosis, we recommend a reexcision procedure for such lesions. The dimensions of such a procedure could follow guidelines for melanoma in situ, or at a minimum should be discussed with the patient and include a margin of normal tissue around the scar and any residual lesion.
|
|
Superficial Spreading Melanoma
Superficial spreading melanoma, also referred to as pagetoid melanoma , is the most frequent form of melanoma (about 70% of all cases), and may therefore be regarded as the "common" or "prototypic" form of melanoma. These lesions were described in the past as "atypical melanocytic hyperplasia" or "precancerous melanosis," a term that dates to one of the earliest descriptions of melanoma by Dubreuilh in 1912 . The lesions, which occur in a relatively young to middle-aged patient population, may occur on exposed skin but are more commonly found on intermittently exposed skin and are rare on unexposed skin. In contrast to lentigo maligna, superficial spreading melanoma is believed to be associated with acute intermittent rather than chronic continuous sun exposure, which is often recreational rather than occupational . The most frequently involved sites are the upper back, especially in men, and the lower legs, especially in women. The lesions are slightly or definitely elevated, with a palpable border and an irregular outline. There is often variation in color that includes not only tan, brown, and black, but also pink, blue, and gray. White areas may be seen at sites of spontaneous regression . Microinvasion may be clinically unapparent, but the onset of tumorigenic vertical growth is indicated by the development of a papule followed by nodularity and sometimes also ulceration, the latter usually a late feature. In rare instances the lesion has a verrucous surface, in which case differentiation from a seborrheic keratosis may be difficult . In its early stage of development, superficial spreading melanoma may be indistinguishable clinically from a dysplastic nevus. Although dermoscopy can improve clinical diagnostic specificity , histologic examination remains the gold standard and is necessary for accurate diagnosis .
|
|
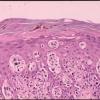
Histopathology.
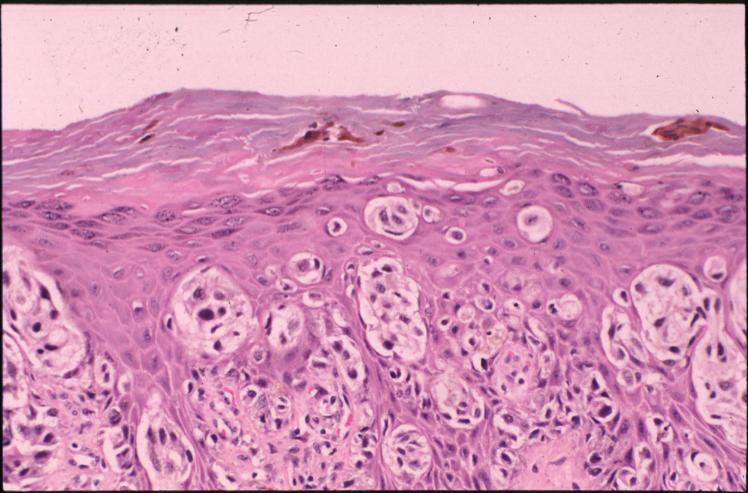
Architectural pattern features of importance in the diagnosis include the large diameter of the lesions, poor circumscription (the last cells at the edge of the lesion tending to be small, single, and scattered), and asymmetry (one half of the lesion does not mirror the other half) . The epidermis is irregularly thickened and thinned, in contrast to the uniformly elongated rete ridge pattern of a dysplastic nevus . Rather uniformly rounded, large melanocytes are scattered in a pagetoid pattern throughout the epidermis. The large cells lie predominantly in nests in the lower epidermis and singly in the upper epidermis. The nests tend to vary a good deal in size and shape and to become confluent. Dermal melanophages and a dermal infiltrate are regularly present. The lymphocytic infiltrate may be patchy and perivascular as in a dysplastic nevus but is typically dense and bandlike, especially in invasive lesions.
|
|
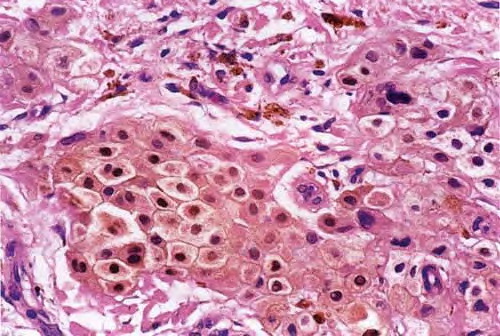
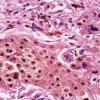
Cytologically, the lesional cells are rather uniform and have abundant cytoplasm containing varying amounts of melanin that often consists of small, "dusty" granules. They are almost entirely devoid of readily visible dendrites. The nuclei tend to be large and hyperchromatic, with irregular nuclear membranes and irregularly clumped chromatin (Fig. 28-20B). This uniform cytologic atypia is of considerable diagnostic importance and contrasts with the random cytologic atypia of dysplastic nevi.
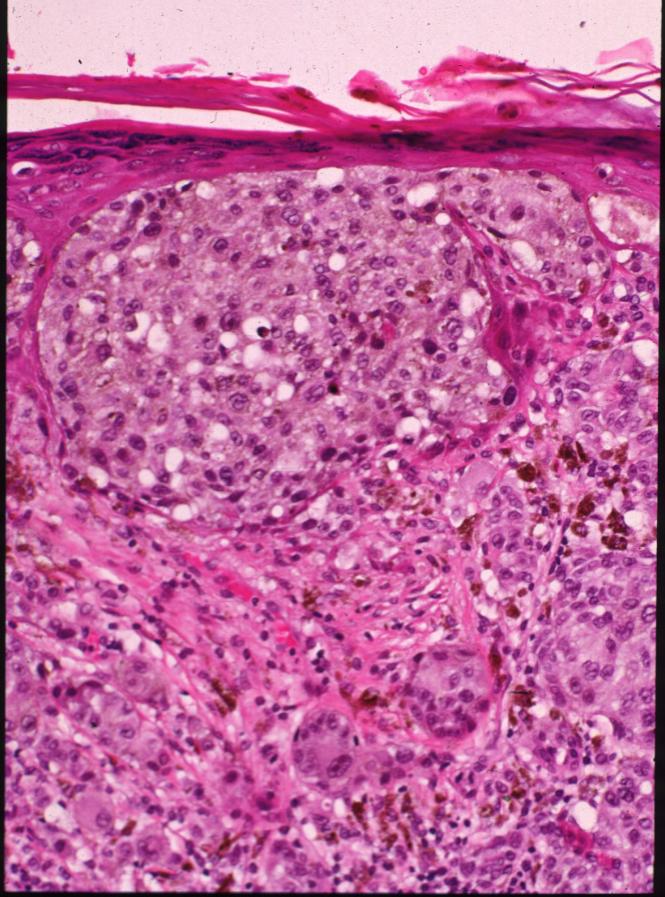
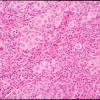
When the lesion is in situ, the basement membrane is intact and there are no lesional cells in the dermis. In an invasive but nontumorigenic lesion (invasive radial growth phase or microinvasive melanoma), cells similar to those in the epidermis are present in the dermis in the form of small nests, with no nests larger than those in the epidermis, and with no dermal mitoses (Fig. 28-20C). When tumorigenic vertical growth phase is present, there is at least one, or often more than one, cluster of cells in the dermis that is larger than the largest intraepidermal nest, and/or there may be lesional cell mitoses in the dermis .
|
|
Histogenesis. On electron microscopic examination, melano-somes are present in great numbers in the large pagetoid tumor cells. Their shape is largely spheroid, rather than ellipsoid as in normal melanocytes and in the tumor cells of lentigo maligna . They often also show other abnormalities, such as absence of cross-linkages of the filaments within the melanosomes. Melanization within the melanosomes is variable but often incomplete . This accounts for the finely divided "dusty" character of the pigment in the cells of many melanomas. As already mentioned, it is likely that most superficial spreading melanomas have mutually exclusive activating mutations of the oncogene BRAF or NRAS. In a recent genotype-phenotype study, melanomas that had prominent nesting and pagetoid scatter of melanocytes-criteria similar to those for superficial spreading melanoma-were
|
|
more likely than other melanomas to be associated with BRAF or NRAS mutations . These evolving genetic data will lead to refinement of the clinicopathologic melanoma classification system in the near future.
|
|
Differential Diagnosis. A junctional nevus differs from superficial spreading melanoma in radial growth phase by a lack of atypia in the tumor cells, particularly in their nuclei, by a lack of pagetoid upward extension of tumor cells, by the absence of a significant inflammatory infiltrate in the upper dermis, and often but not always by a sharper lateral demarcation. Salient features in the important distinction from junctional melanocytic dysplasia have been reviewed , and include, at scanning magnification, larger size, asymmetry, an irregularly thickened and thinned epidermis, and a bandlike lymphocytic infiltrate in superficial spreading melanoma. At higher power, indicators of melanoma include the presence of high-level and extensive pagetoid melanocytosis (large neoplastic cells scattered among benign keratinocytes), high-grade and/or uniform cytologic atypia, and lesional cell mitoses (the latter present in about one third of cases). A junctional Spitz nevus, especially the uncommon pagetoid Spitz nevus, may simulate superficial spreading melanoma quite closely. Distinguishing features include generally smaller size, the presence of large spindle and/or epithelioid cells, the presence of Kamino bodies, and the lack of "consumption" or thinning of the epidermis above the lesion, as previously discussed (see section Spitz Nevus). The so-called nevi of special sites, including flexural sites, ears, scalp, and breast, may also simulate this form of melanoma in particular, and these should be seriously considered when a biopsy from one of these sites is examined (see also page 715). Caution should be exercised when what at first appears as melanoma in situ is restricted to the epidermis that overlies a surgical or traumatic scar because this must be differentiated from the recurrent nevus phenomenon [see section Recurrent Nevus (Pseudomelanoma)]. Helpful features include the precise spatial restriction of the atypical intraepidermal focus to the zone overlying (but not extending horizontally beyond) the scar, the presence of residual nevus cells, and the absence of true uniform cytologic atypia. Whenever possible, it is important to also review the initial biopsy in such cases. The differential diagnostic distinction from lentiginous melanomas is of less consequence because the management is the same. In lentigo maligna, the epidermis is atrophic and pagetoid melanocytosis is less prominent, and contiguous replacement of the basal cell layer by atypical melanocytes is the dominant pattern. Problematic cases can be reported as malignant melanoma (in situ or microinvasive, etc.) without designation as to type.
|
|
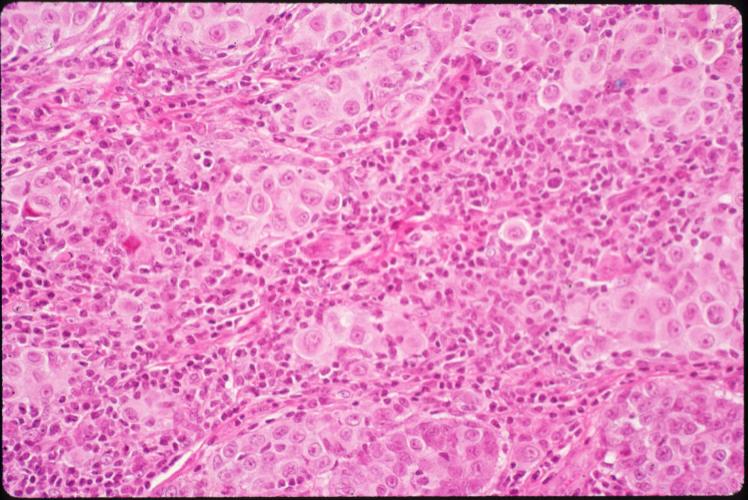
When tumorigenic vertical growth phase is present, it does not differ appreciably from that in any other form of melanoma, except for the adjacent radial growth phase . Classification of such complex tumorigenic primary melanomas is based on the morphology of the radial growth phase.
|
|
Among the nonmelanocytic neoplasms that must be differentiated from a superficial spreading melanoma in situ are Paget's disease and pagetoid examples of Bowen's disease (squamous cell carcinoma in situ). Paget's disease usually shows remnants of compressed basal cells beneath the tumor cells, whereas in superficial spreading melanoma the lesional cells extend to the basement membrane. In Paget's disease, the tumor cells may stain positively for carcinoembryonic
|
|
antigen and keratin and are negative for HMB-45 and Melan-A. S100 reactivity, although unusual, may occasionally be observed in Paget's disease. Pagetoid Bowen's disease (discussed in Chapter 29) shows, as a rule, a wellpreserved basal cell layer, except in areas in which dermal invasion has taken place, and immunohistochemically the atypical cells stain positively with antikeratin antibodies (e.g., AE1/AE3) . They do not stain with S100 or with Melan-A or HMB-45. It should be noted that the cells of Paget's disease and of Bowen's disease may contain melanin pigment because of transfer from reactive melanocytes in the adjacent skin.
|
|
A final pitfall in evaluating nonmelanocytic mimics of intraepidermal melanoma involves the variable tendency of keratinocytes within the uppermost epidermal layers to exhibit perinuclear retraction presumably due to cytoplasmic glycogenation combined with tissue processing. Some body sites (e.g., areola and along the milk line) may be particularly prone to this change, perhaps in part the result of so-called "clear cells of Toker." These cells may produce the false appearance of true pagetoid spread in an otherwise benign or dysplastic melanocytic lesion, thus inciting consideration of a diagnosis of superficial spreading melanoma. However, keratinocytes so altered are recognizable at high magnification as cells with nuclei surrounded by clear spaces (retraction clefts) that themselves are bordered by a rim of cytoplasm and joined by desmosomes, in contrast to pagetoid melanoma cells, which lack desmosomes and whose nuclei are directly enveloped by relatively clear cytoplasm that may be surrounded by a thin, clear mantle of retraction that separates the cell from adjacent keratinocytes.
|
|