|
Melanocytic Nevi
Common Melanocytic Nevus
Although the term "nevus" may refer to a variety of hamartomatous and/or neoplastic lesions in the skin, the unqualified term in common usage and in this chapter refers to a melanocytic nevus, which is generally considered to be a benign neoplastic proliferation of melanocytes, leading to a localized pigmented or nonpigmented lesion usually less than 5 mm in diameter. Nevi vary considerably in their clinical appearance. In addition to the pathologic variants, which will be discussed separately, five clinical types may be recognized: (a) flat lesions, (b) slightly elevated lesions, often with a raised center and a flat periphery, (c) papillomatous lesions, (d) domeshaped lesions, and (e) pedunculated lesions. The first three types are always pigmented; the last two mayor may not be pigmented. Any of the elevated lesions may be surrounded by a flat periphery, within which changes of melanocytic dysplasia may be seen histologically ("nevus with dysplasia"). Dome-shaped lesions often contain several coarse hairs. Although exceptions occur, one can predict to a certain degree from the clinical appearance of a nevus whether on histologic examination it will prove to be a junctional nevus (confined to the epidermis), a compound nevus (epidermal and dermal), or an intradermal nevus. Most small, flat lesions represent either a lentigo simplex or a junctional nevus; flat lesions or lesions with a flat periphery 5 mm or more in diameter with irregular indefinite borders and pigment variegation are clinically dysplastic nevi, although if these changes are severe, melanoma may need to be ruled out. Most slightly elevated lesions and some papillomatous lesions represent compound nevi (especially if they are pigmented); and most papillomatous lesions and nearly all domeshaped and pedunculated lesions that are not pigmented represent intradermal nevi .
|
|
Melanocytic nevi are only rarely present at birth (see section Congenital Melanocytic Nevus). Most nevi appear in adolescence and early adulthood. In this age period, they may occur episodically and, rarely, as widespread eruptive nevi . New nevi arise occasionally in midlife and rarely in later life. Except for occasional cosmetic significance, nevi are important only in relation to melanoma, for which they are risk markers, simulants, and potential precursors .
|
|
A general concept of clinical importance for melanocytic nevi is that, unlike melanoma, which inexorably progresses over time, nevi enlarge to a point, stabilize, and then involute, becoming less frequent in the elderly than in younger age groups . This clinical attribute is directly related to the importance of heightened suspicion that is aroused when a previously stable nevus undergoes change in size or pigmentation.
|
|
Histopathology
Melanocytic nevi are defined and recognized by the presence of nevus cells, which, even though they are melanocytes, differ from ordinary melanocytes by being arranged at least partially in clusters or "nests." Other defining characteristics of nevus cells include a tendency to rounded rather than dendritic cell shape and a propensity to retain pigment in their cytoplasm rather than to transfer it to neighboring keratinocytes . Nevus
|
|
cells show considerable variation in their appearance and often are not pigmented, so that they are often recognizable as nevus cells more by their arrangement in clusters or nests than by their cellular features. As the result of a characteristic shrinkage artifact, nevus cell nests often appear partially separated from their surrounding stroma and, in some nevi such as the spindle and epithelioid cell variant, from surrounding epithelium.
|
|
Although a histologic subdivision of nevi into junctional, compound, and intradermal nevi is generally accepted, it should be realized that these are transitional stages in the life cycle of nevi, from junctional to compound to intradermal, and finally to involuting lesions.
|
|
Lentigo Simplex. Lentigo simplex, as described earlier, may be regarded as an early or evolving form of melanocytic nevus. Histologically, these are small (usually less than 2 mm) and are characterized by an increased number of nevoid melanocytes present in contiguity with one another near the tips and sides of elongated rete ridges. This pattern, characteristic of lentigines, is therefore described as lentiginous melanocytic proliferation. The lack of nests at the histologic level distinguishes the lentigo from a nevus, by definition. However, transitional forms between a simple lentigo and a lentiginous junctional nevus (a lentigo with a few nests) are commonly observed, and the two histologic entities are indistinguishable clinically, giving rise to the term nevoid lentigo or jentigo . The former term has been used more or less synonymously with lentigo maligna , and therefore we prefer the term lentiginous junctional nevus for these very common lesions .
|
|
Junctional Nevus. In a junctional nevus, nevus cells may lie in well-circumscribed nests either entirely within the lower epidermis or bulging downward into the dermis but still in contact with the epidermis, perhaps in the process of dropping off to form a compound nevus. The nevus cells in these nests generally have a regular, rounded to cuboidal appearance, although they are occasionally spindle shaped. In addition, a varying number of diffusely arranged single nevus cells is seen in the lowermost epidermis, especially in the basal cell layer. In many lesions, single cells are about as common as nests, recapitulating the histology of a simple lentigo. Such lesions in our practice are termed lentiginous junctional nevi . Varying amounts of melanin granules are seen in the nevus cells. Some of the nevus cells, on staining with silver, show dendritic processes containing melanin granules, making them indistinguishable from melanocytes, but in general the degree of dendritic differentiation is markedly reduced compared to melanocytes. The nested and single melanocytes are arranged mainly at the tips and sides of rete ridges; continuous proliferation of single cells between the rete, confluence of nests, or pagetoid extension of cells into the suprabasal epidermal layers may be architectural indicators of dysplasia or evolving in situ melanoma.
|
|
Although nevus cells only occasionally penetrate into the upper layers of the epidermis ("pagetoid extension"), aggregates
|
|
of melanin granules may be seen in the stratum corneum in deeply pigmented junctional nevi. Often, the rete ridges are elongated as in lentigo simplex (see section Lentigo Simplex and Related Lesions), and single cells, as well as nests of nevus cells, are seen at the bases of the rete ridges. Not infrequently, as in lentigo simplex, the upper dermis contains an infiltrate of melanophages and mononuclear cells. These lesions that combine features of lentigo simplex and junctional nevus are exceedingly common, and, as indicated, may be termed lentiginous junctional nevi. Lesions with these features but larger than 5 mm clinically or 4 to 5 mm in a histologic section
|
|
often prove to have cytologic atypia and to be dysplastic nevi (see section Dysplastic Nevus).
|
|
In children, some junctional nevi may show considerable cellularity with some degree of cellular enlargement, pleomorphism, and pagetoid cells above the basal layer. They may also often show fine, dusty melanin particles and a dense inflammatory infiltrate (92,108). Some of these lesions may represent Spitz nevi or dysplastic nevi (see respective sections). Others may correlate with a tendency for ordinary junctional nevus cells to be enlarged, or epithelioid, in younger individuals. The small size of the lesion, the sharp lateral demarcation, the lack of severe or uniform atypia and of mitoses, and the fact that in children melanomas are very rare help in the distinction from melanoma. However, if the criteria mentioned are present, the diagnosis of melanoma should be considered, even in a child.
|
|
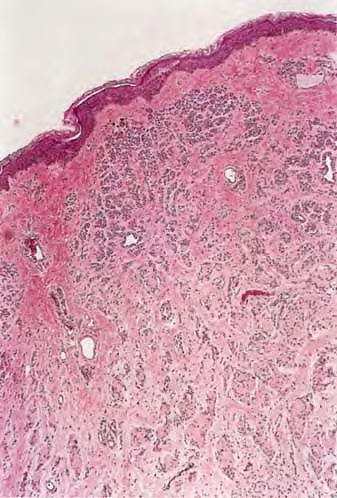
Compound Nevus. Clinically, a compound nevus is a pigmented papule or a plaque. In most nondysplastic
|
|
compound nevi, there is no adjacent macular component. Histologically, a compound nevus possesses features of both a junctional and an intradermal nevus. Nevus cell nests are present in the epidermis, as well as appearing to "drop off' from the epidermis into the superficial dermis and, in many lesions, the reticular dermis . This time-honored theory of abtropfung or dropping off of nevus cells proposed by Unna has been challenged by the finding that junctional nevi are at least as common in adults as in children . Nevus cells in the upper, middle, and lower dermis may present characteristic morphologic variations called types A, B, and C, respectively . Usually, the type A nevus cells in the upper dermis are round to cuboidal, show abundant cytoplasm containing varying amounts of melanin granules, and tend to form nests. Type A cells with especially abundant cytoplasm, as may occur in children and young adults, may be termed epithelioid cells . Melanophages are occasionally seen in the surrounding stroma. The cells in the mid dermis usually are type B cells; they are distinctly smaller than the type A cells, display less cytoplasm and less melanin, and generally lie in well-defined aggregates or cords. They may to some extent resemble lymphoid cells (Fig. 28-60). Type C nevus cells in the lower dermis tend to resemble fibroblasts or Schwann cells because they are usually elongated and possess a spindle-shaped nucleus. They often lie in strands and only rarely contain melanin . Occasionally they form aggregates that resemble Meissner corpuscles. Occasional nevi show abnormal stratification within the deeper dermis of otherwise benign type A nevus cells, resulting in the designation of inverted type A nevus.
|
|
The decrease in cell size, melanization, and progression from nests to cords to more neuroid spindle cells with dermal descent seen in nevi is often referred to as maturation and is regarded as evidence of benignity because the size of the cells in a melanoma usually does not decrease with depth. The process of nevus cell maturation has alternatively been regarded as one of senescence or atrophy , perhaps driven by the tumor suppressor p16, which is activated in response to the effects of an activated oncogene such as BRAF or NRAS in a phenomenon termed oncogene-induced senescence . If dermal nevus cells are confined to the papillary dermis, they often retain a discrete or "pushing" border with the stroma. However, nevus cells that enter the reticular dermis tend to disperse among collagen fiber bundles as single cells or attenuated single
|
|
files of cells. This pattern of infiltration of the dermis differs from that in most melanomas, in which groups of cells tend to dissect and displace the collagen bundles in a more expansive pattern (113). Lesions in which nevus cells extend into the lower reticular dermis and the subcutaneous fat or are located within nerves, hair follicles, sweat ducts, and sebaceous glands may be termed congenital pattem nevi because they share morphologic features with congenital nevi but are not necessarily present at birth .
|
|
Intradermal Nevus.
Intradermal nevi show essentially no junctional activity. The upper dermis contains nests and cords of nevus cells. Multinucleated nevus cells may be seen in which small nuclei lie either in a rosette-like arrangement or close together in the center of the cell. These nevus giant cells differ significantly in appearance from the irregularly and even bizarrely shaped giant cells that are seen frequently in Spitz nevus and occasionally also in melanoma. As a result of shrinkage during tissue processing, clefts may form between some nests of nevus cells and the surrounding epidermis, as well as stroma, the latter leaving a defect that simulates a lymphatic space and thus mimics lymphatic invasion
|
|
Whereas the nevus cell nests located in the upper dermis often contain a moderate amount of melanin (particularly type A cells), the type Band C nevus cells in the mid portion and the lower dermis rarely contain melanin. Type C cells appear spindle shaped, are arranged in bundles, and are embedded in collagenous fibers having a loose, pale, wavy appearance similar to that of the fibers in a neurofibroma, resulting in a "neurotized nevus." Such formations have been referred to as neuroid tubes. In other areas, the nevus cells lie within concentrically arranged, loosely layered filamentous tissue, forming so-called nevic corpuscles that resemble Meissner's tactile bodies . Neurotized nevus cells express the marker S100A6 protein, a form of S100 found in Schwann cells, supporting the hypothesis that maturation in these lesions recapitulates some features of Schwann cell differentiation .
|
|
Occasional intradermal nevi are devoid of nevus cell nests in the upper dermis and contain only spindle-shaped nevus cells embedded in abundant, loosely arranged collagenous tissue. These nevi may be referred to as neural nevi. The differentiation from a solitary neurofibroma may be difficult in routinely stained sections, but distinction might be possible with an immunohistochemical technique using myelin basic protein, which is positive only in neurofibroma (see Histogenesis). Neurofibromas also tend to contain small nerve twigs and axons that can be highlighted with glial fibrillary acidic protein staining , a feature not typical of neurotized nevi.
|
|
Some intradermal and, less commonly, compound nevi show hyperkeratosis and papillomatosis, which may be associated with a lacelike, downward growth of epidermal strands and with hom cysts. Such nevi resemble seborrheic keratoses in their epidermal architecture. In other instances, large hair follicles are observed. Rupture of a large hair follicle may manifest itself clinically in an increase in the size of the nevus associated with an inflammatory reaction, leading to clinical suspicion of a melanoma. Histologic examination in such instances shows a partially destroyed epidermal follicular lining with a pronounced inflammatory infiltrate containing foreignbody giant cells as a reaction to the presence of keratin in the dermis. Occasionally, intradermal nevi contain scattered large fat cells within the aggregates of nevus cells. This is likely to be a regressive phenomenon in which fat cells replace involuting nevus cells or, alternatively, (and more likely) true adipocyte metaplasia within the stroma of the nevus.
|
|
Some intradermal nevi, including variants of spindle and epithelioid cell nevi, induce marked deposition of coarse, sometimes hyalinized collagen. Such nevi are described as sclerosing variants. This change occasionally may confound diagnosis but is not of biological significance.
|
|
In occasional otherwise typical dermal nevi (or in the dermal component of compound nevi), rare mitoses are found in the dermis. This phenomenon has been described in children and in association with pregnancy . If there are no other indicators of malignancy, we report these cases as "nevi with mitoses" and generally recommend complete excision. The possibility of nevoid melanoma (see later section) should be seriously considered in such lesions .
|
|
Pathogenesis of Acquired Melanocytic Nevi
For many years, Masson's theory of the dual origin of nevus cells was widely accepted . He believed that the nevus cells in the upper dermis developed from epidermal melanocytes, whereas the nevus cells in the lower dermis developed from Schwann cells, as suggested by the frequent presence of nervelike structures in the latter. The fact that both melanocytes and Schwann cells are derived from the neural crest seemed to support Masson's view, as did the presence of a nonspecific cholinesterase reaction in both deep nevus cells and Schwann cells and the absence of melanin in the deep nevus cells . However, in favor of a melanocytic origin of these deep dermal nevus cells was the presence of melanosomes with dopa-oxidase activity even in deeply situated nevus cells that had a neuroid appearance on light microscopy . An electron microscopic examination of neuroid structures in nevi revealed that these nevic corpuscles contained no Schwann cells or axons but were instead composed exclusively of cells that contain premelanosome-like dense bodies in their perikaryon . Furthermore, myelin basic protein has been found to be regularly present by immunoperoxidase in Schwann cells and absent in all types of melanocytic nevi . In addition, melanocyte-specific markers like Melan-AIMART-1, HMB-45, tyrosinase, and others are often positive in nevi but typically absent in neural cells and neurofibromas .
|
|
Another important point in favor of a single origin of the nevus cell is to be found in the life cycle of nevi. Although there are exceptions, most nevi appear in childhood, adolescence, and early adulthood, and, with advancing age, there is a progressive decrease in the number of nevi . The evolution and involution of nevi correlate with their histologic appearance. Junctional proliferation of nevus cells is present in almost every
|
|
nevus in children but decreases with age. Intradermal nevi, by contrast, are most unusual in the first decade of life, and their proportion increases progressively with age. The incidence of fibrosis, fatty infiltration/metaplasia, and neuroid changes increases with age. Thus, the formation of cylindrical neuroid structures represents the end stage of differentiation and not a source of origin of intradermal nevi .
|
|
Concerning the relationship between epidermal melanocytes and nevus cells, some authors believe that these two types of cells have a different embryologic genesis, with the nevus cell originating from a neural crest precursor cell referred to as a nevoblast . Most authors regard the two cell types as identical, however . It would seem that the morphologic features by which nevus cells differ from melanocytes, such as the absence of dendrites as seen by light microscopy, their arrangement in cell nests, their larger size, and their tendency to retain pigment, are secondary adjustments of the cells. Electron microscopy has shown that the fine structure of nevus cells is comparable to that of epidermal melanocytes (EM 46, 47). Cultured nevus cells, whether derived from congenital or acquired lesions, have been found to be highly dendritic, as are epidermal melanocytes . In conclusion, it seems established that nevus cells differ from Schwann cells and are benign neoplastic variants of melanocytes.
|
|
The molecular pathology of nevi is beginning to be understood. In a recent study of the BRAF oncogene, which had previously been found to be mutated in a high percentage of metastatic melanomas , mutations resulting in the V599E amino acid substitution were found in 68% of melanoma metastases, 80% of primary melanomas, and, unexpectedly, 82% of nevi (132). Activating mutations of the oncogene NRAS (mutually exclusive with BRAF mutations) have also been described in melanoma-associated nevi and in congenital nevi . These data suggest that mutational activation of the RAS/RAF/MAPK mitogenic pathway in nevi is a critical step in the initiation of melanocytic neoplasia but alone is insufficient for melanoma tumorigenesis . High levels of the tumor suppressor gene product p161NK4 in benign nevi may represent the mechanism whereby the cell cycle remains regulated in nevi, even in the presence of activating oncogene mutations .
|
|