ERYSIPELAS
Erysipelas is a distinct type of superficial cutaneous cellulitis with marked dermal lymphatic vessel involvement caused by group A β-hemolytic streptococcus (very uncommonly group C or G streptococcus) and rarely caused by S. aureus. In the newborn, group B streptococci can cause erysipelas. Lymphedema, venous stasis, web intertrigo, and obesity are risk factors in the adult patient.
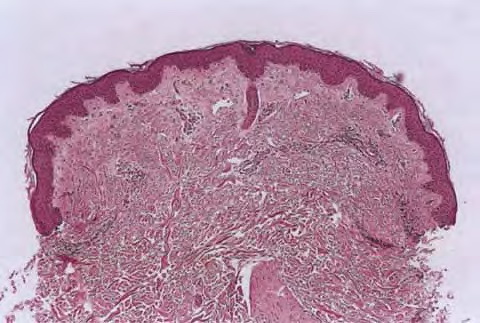
In the absence of underlying edema or other skin abnormalities, erysipelas
usually begins on the face or a lower extremity, heralded by pain, superficial erythema, and plaque-like edema with a sharply defined margin to normal tissue . These findings are often described as peau d'orange appearance. In the presence of antecedent edema or other anatomic abnormalities, the margin between normal and diseased soft tissue may be obscure, much as in primary cellulitis. There may not be an obvious portal of entry, and skipped areas may confuse the nature of the process. Facial erysipelas is less frequent than lower extremity disease and begins unilaterally but may spread by contiguity over the nasal prominence to involve the face symmetrically . The oropharynx may be a portal of entry, and throat culture may show GAS. Inflammatory edema may extend to the eyelids, but orbital complications are rare. Fever may precede local signs, and, occasionally, before distal extremity
findings, patients complain of groin pain caused by swelling of a femoral node. Lymphangitis and abscess are very rare, but the process may spread rapidly from the initial lesion. Occasionally, in addition to rapid spread of the erythematous, edematous plaque, bullae may form in the involved area.
Etiology of Soft-Tissue Infections
|
|
TYPE OF INFECTION
|
MOST COMMON CAUSE(S)
|
UNCOMMON CAUSES
|
|
Erysipelas
|
Group A streptococcus
|
Group B, C, and G streptococcus, Staphylococcus aureus
|
|
Cellulitis
|
S. aureus, group A streptococcus
|
Group B, C, and G streptococcus; Streptococcus iniae; Pneumococcus; Haemophilus influenzae (children); Escherichia coli; Proteus, other Enterobacteriaceae; Campylobacter jejuni; Moraxella; Cryptococcus neoformans; Legionella pneumophila, L. micdadei; Bacillus anthracis (anthrax); Aeromonas hydrophila; Erysipelothrix rhusiopathiae; Vibrio vulnificus, V. alginolyticus, V. cholerae non-01
|
|
Cellulitis in children
|
S. aureus, group A streptococcus
|
Group B streptococcus (neonates)
|
|
|
Facial/periorbital cellulitis
|
S. aureus, group A streptococcus
|
Neisseria meningitides, H. influenzae (young children)
|
|
|
Perianal cellulitis
|
Group A streptococcus
|
S. aureus
|
|
Cellulitis second degree to bacteremia
|
Pseudomonas aeruginosa
|
V. vulnificus; S. pneumoniae; group A, B, C and G streptococcus
|
|
Crepitant cellulitis
|
Histotoxic Clostridia sp., (C. perfringens, C. septicum)
|
Bacteroides sp.; Peptostreptococci; E. coli, Enterobacteriaceae
|
|
Cellulitis associated with water exposure
|
E. rhusiopathiae (erysipeloid)
|
V. vulnificus, Aeromonas hydrophila, Mycobacterium marinum (nodular lymphangitis), M. fortuitum complex
|
|
Gangrenous cellulitis (infectious gangrene)
|
|
|
|
|
NF
|
|
|
|
|
|
Streptococcal gangrene
|
Group A streptococcus
|
Groups B, C, and G streptococcus
|
|
|
|
Nonstreptococcal NF
|
Mixed infection with one or more anaerobes (Peptostreptococcus or Bacteroides) plus at least one facultative species (non-group A streptococci; members of the Enterobacteriaceae such as Enterobacter, Proteus, etc.)
|
|
|
|
|
Synergistic necrotizing cellulitisa
|
Polymicrobial with facultative and anaerobic organisms that originate in the intestine; one-third of patients have positive blood cultures, usually a coliform, Bacteroides, or Peptostreptococcus
|
|
|
|
|
|
Facultative
|
Coliforms: E. coli, Proteus, Klebsiella
|
|
|
|
|
|
Anaerobes
|
Bacteroides, Peptostreptococcus, Clostridium, Fusobacterium
|
|
|
|
|
Fournier gangrene
|
Similar to nonstreptococcal NF (type I)
|
|
|
|
Clostridial soft-tissue infections
|
C. perfringens, other histotoxic clostridial species
|
|
|
|
|
Anaerobic cellulitis
|
|
|
|
|
Anaerobic myonecrosis (gas gangrene)
|
|
|
|
|
|
Spontaneous, nontraumatic anaerobic myonecrosis
|
C. septicum (bacteremic)
|
|
|
|
Nonclostridial anaerobic cellulitis
|
Various Bacteroides sp., peptostreptococci, peptococci
|
|
|
|
Progressive bacterial synergistic gangrene (Meleney gangrene)
|
Mixed bacterial infection
|
|
|
|
|
Ulcer base
|
S. aureus
|
Proteus sp., other Gram-negative bacilli
|
|
|
|
Advancing margin
|
Microaerophilic or anaerobic streptococci
|
|
|
|
Gangrenous cellulitis in the immunosuppressed individual
|
P. aeruginosa (ecthyma gangrenosum) Mucor, Rhizopus, Aspergillus
|
Bacillus sp., other bacterial and fungal sp.
|
|
a Essentially the same as nonstreptococcal necrotizing fasciitis (NF) but with some involvement of adjacent skeletal muscle.
|
|
Recurrent erysipelas is associated with saphenous vein harvest (occasionally in association with tinea pedis) and lymphedema complicating mastectomy with axillary node dissection. In these cases, erysipelas presents with edema and erythema along lines of venectomy or nodal dissection. In addition, resultant lymphedema from a previous episode of erysipelas is a risk factor for recurrence, particularly on the lower extremities. Congenital lymphedema (Milroy disease) may also lead to recurrent erysipelas.
|