|
Dermatomyositis
Dermatomyositis manifests as an inflammatory myopathy with characteristic cutaneous findings. In the absence of cutaneous findings, the diagnosis of polymyositis is applied. Cutaneous findings alone, without muscular involvement, have been termed amyopathic dermatomyositis or dermatomyositis sine myositis (.
|
|
Both dermatomyositis and polymyositis are uncommon diseases that have a similar incidence. Both have two peaks of occurrence: one in childhood and one between the ages of 45 and 65 years . In some instances, the cutaneous eruption precedes the development of muscular weakness by many months or even several years.
|
|
The four systemic and single cutaneous diagnostic criteria for dermatomyositis are symmetric proximal muscle weakness, elevated muscle enzymes, an abnormal electromyelogram in the absence of neuropathy, consistent muscle biopsy changes, and cutaneous findings . Involvement of the skeletal muscles causes progressive weakness, vague muscular pain, and, later, muscle atrophy. The proximal muscles of the extremities and the anterior neck muscles often are the first to be involved. Involvement of the pharynx may result in dysphagia and aspiration of food, and involvement of the diaphragm and the intercostal muscles may lead to respiratory failure. Arthritis and arthralgias may occur in up to 25% of cases. Other, less common systemic manifestations, such as interstitial pneumonitis, dysphagia, dysphonia, and cardiac conduction abnormalities, portend a worse prognosis.
|
|
Two distinctive cutaneous lesions are found in dermatomyositis. One is violaceous, slightly edematous periorbital patches that primarily involve the eyelids, known as the heliotrope rash. The other is discrete red-purple papules
|
|
over the bony prominences, particularly the knuckles, knees, and elbows, known as Gottron's papules. These may evolve into atrophic plaques with pigmentary alterations and telangiectasia and are then known as Gottron's sign.
|
|
Other cutaneous findings include periungual telangiectasia, hypertrophy of cuticular tissues associated with splinter hemorrhages, photosensitivity, and poikiloderma. Often lesions resembling the erythematous-edematous lesions seen in subacute cutaneous or systemic lupus erythematosus may be found. Subcutaneous and periarticular calcification may be found, particularly in affected children. Calcinosis is usually seen centered in the proximal muscles of the shoulders and pelvic girdle. Childhood onset may also be associated with lipodystrophy and insulin resistance {68}. Other uncommonly reported cutaneous findings include gingival telangiectasia, angiokeratomas, panniculitis, flagellate erythema, scleromyxedematous lesions, and pityriasis rubra pilaris-like lesions .
|
|
Controversy exists over the association of dermatomyositis with malignancy . Interpretation of reports with incidences of 6% to 50% is hampered by the asynchronous development of malignancy in relation to the dermatomyositis. Some series fail to show a significant difference between affected patients and the control population. If malignancy arises with dermatomyositis, it usually occurs in the adult form. Some sources indicate that this association is also present in the childhood form, whereas others view such reports with skepticism. Various tumors have been reported, with ovarian carcinoma perhaps being most frequent . Larger populationbased studies have suggested an incidence of carcinoma at between 20% and 25% . Although ovarian carcinoma is still considered the most common associated malignancy, other tumors reported include lung, prostatic, pancreatic, and gastrointestinal carcinomas. In younger males, testicular carcinoma is more prevalent. In Asians, there is an increased association with nasopharyngeal carcinoma .
|
|
As with lupus erythematosus, the pathogenesis of the disease is uncertain. Associated antibodies include PM1, J01 {correlates with pulmonary fibrosis}, Ku {associated with sclerodermatomyositis}, and M2. Other recently reported markers include autoantibodies to 155kd, and Se antigens have been reported to be associated with amyopathic dermatomyosis. . A single case of a cutaneous eruption mimicking dermatomyositis after treatment with imatinib mesylate has
|
|
been reported . Medications including hydroxyurea, quinidine, nonsteroidal antiinflammatory agents, dpenicillamine, isoniazid, and 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors have been reported to exacerbate dermatomyositis.
|
|
On the whole, the prognosis of dermatomyositis is favorable, especially when treatment with corticosteroids is used. Other therapeutic agents include methotrexate, azathioprine, cyclophosphamide, mycophenolate mofetil, chlorambucil, and cyclosporine. The mortality has been reported to be approximately 14% in some series, with metastatic malignancy a frequent cause of death .
|
|
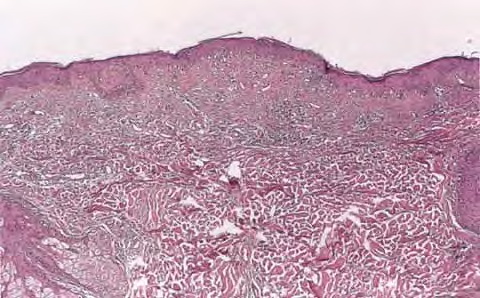
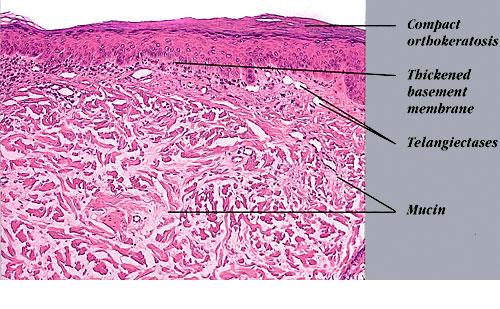
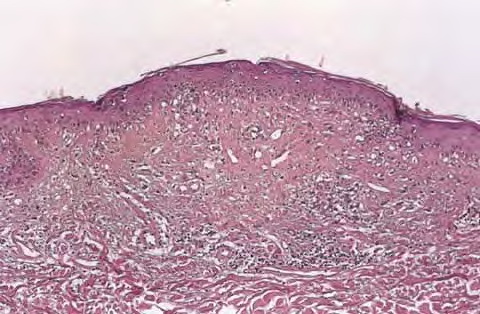
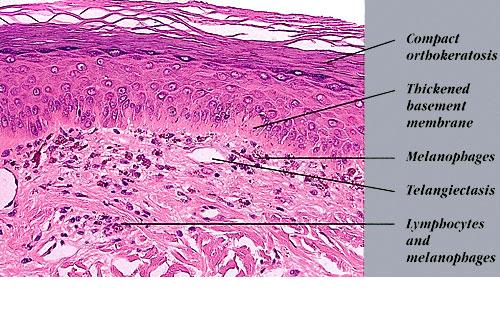
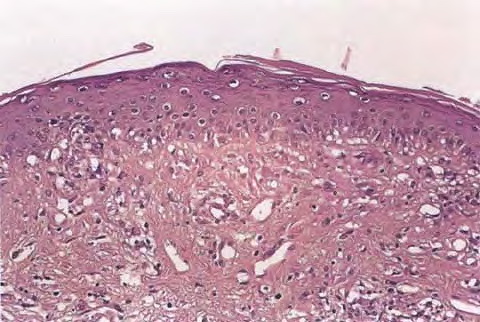
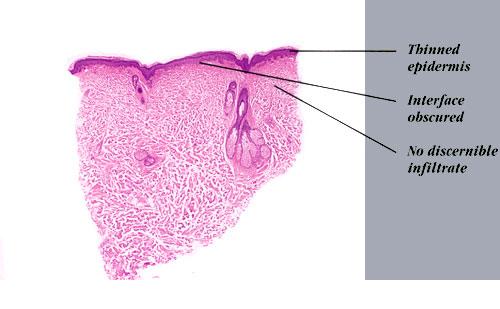
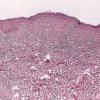
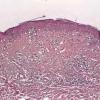
Histopathology. The erythematous-edematous lesions of the skin in dermatomyositis may show only nonspecific inflammation. However, quite frequently the histologic changes are indistinguishable from those seen in SLE. There is epidermal atrophy, basement membrane degeneration, vacuolar alteration of basilar keratinocytes, a sparse lymphocytic inflammatory infiltrate around blood vessels, and interstitial mucin deposition . With severe inflammatory changes, there may be associated subepidermal fibrin deposition. Although immune complexes are not detected at the dermal-epidermal junction as in lupus erythematosus, it should be
|
|
remembered that up to 50% of subacute cutaneous lupus biopsies can also have a negative direct immunofluorescence.
|
|
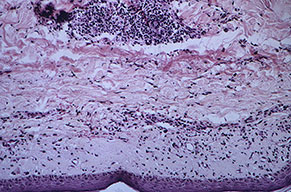
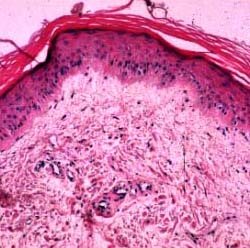
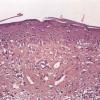
Old cutaneous lesions with the clinical appearance of poikiloderma atrophicans vasculare usually show a bandlike infiltrate under an atrophic epidermis with hydropic degeneration of the basal cell layer (see also the section on poikiloderma atrophicans vasculare). The Gottron's papules overlying the knuckles also show vacuolization of the basal cell layer but acanthosis rather than epidermal atrophy . Subcutaneous tissue may show focal areas of panniculitis associated with mucoid degeneration of fat cells in early lesions. Extensive areas of calcification may be present in the subcutis at a later stage .
|
|
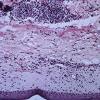
Magnetic resonance imaging permits noninvasive assessment of muscle inflammation and may serve as a guide in locating a site for muscle biopsy. Tender proximal muscles of an extremity yield more useful information than atrophic, weak muscles, which show end-stage changes. Three types of changes may be observed in active disease: (a) interstitial inflammatory infiltrates composed of lymphocytes and macrophages, (b) segmental muscle fiber necrosis (loss of skeletal muscle transverse striation, hyalinization of the sarcoplasm, fragmentation andlor phagocytosis of degenerated muscle fragments), or (c) vasculopathy . The latter entity may be seen in the childhood form and shows immunocomplex deposition in vessel walls . Old lesions usually show a rather nonspecific picture of atrophy of the muscle fibers and diffuse interstitial fibrosis with relatively little inflammation.
|
|
Systemic Lesion
s. Changes in organs other than the skin and the striated muscles occur only rarely in dermatomyositis, in contrast to SLE and systemic scleroderma. The myocardium may show changes identical to those in the skeletal muscle but less severe. Ulcerative lesions in the gastrointestinal tract, caused by vascular occlusions, have also been described .
|
|
Histogenesis. On electron microscopic examination the degenerative changes include focal disintegration of myofilaments and myofibrils, vacuolization, and accumulation of lipid and Iysosomes within muscle fibers. As in lupus erythematosus, nonspecific intracytoplasmic tubuloreticular structures may be found in skin and muscles.
|
|
Differential Diagnosis
. Differentiation of the cutaneous lesions of dermatomyositis from those of subacute cutaneous or systemic lupus erythematosus may be impossible on a histologic basis. It may also be impossible on clinical grounds in cases in which muscular weakness is mild or absent, as it may be in the early stage of dermatomyositis. In such cases, laboratory tests are of great value. The most important is the
|
lupus band test, which is always negative in lesions of dermatomyositis , whereas in lesions oflupuserythematosus it is positive in 90% of the cases. Other tests that are usually negative indermatomyositis and often positive in lupus erythematosus include urinalysis and renal function tests,as well as tests for antinuclear antibodies, anti-native DNA antibodies, and antibodies to ribonucleoprotein. Rarely, patients with dermatomyositis demonstrate a positive Ro antibody titer.Patients with active myositis show an elevation of serum creatine kinase and aldolase
|