|
Atopic Dermatitis
The eruption in atopic dermatitis is characterized by areas of severe pruritus, erythema, scaling, and excoriation, with chronicity, lichenification, and lichen simplex chronicus. Many of the cutaneous changes are due to chronic
|
|
rubbing and scratching. Most patients are diagnosed in childhood, with approximately one third of cases diagnosed before 1 year of age . There is a female predominance, and many patients have other atopic disorders such as allergic rhinitis or asthma. Increased incidence of contact dermatitis is also noted among patients with atopic dermatitis. In infants, the lesions predominate on the face and extensor surfaces of the extremities, but they later affect the flexural surfaces. The classically involved sites in older children and adults are the popliteal and antecubital fossae and the sides of the neck. Secondary bacterial infection is common.
|
|
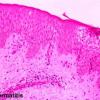
Histopathology.
In early phases, there is mild spongiosis, exocytosis of lymphocytes, and parakeratosis. Lymphocytes and scattered histiocytes are present around the superficial vascular plexus. In long-standing lesions, the rete ridges are regularly elongated, with less prominent spongiosis and cellular infiltrate. Hyperkeratosis and wedge-shaped hypergranulosis with areas of parakeratosis develop. There appear to be an increased number of small vessels with thickened walls. Eosinophils are less conspicuous than in allergic contact or nummular dermatitis. With time, the changes may be those of lichen simplex chronicus.
|
|
Pathogenesis
The current understanding of the disease remains incomplete. Atopic dermatitis develops as a result of complex interactions of genetic, environmental, and immunologic factors. Allergic reactions appear to play a role in some patients, but in other patients, factors such as disturbance of skin function, infection, and stress may be more important. Atopic dermatitis can be exacerbated by fungal, bacterial, and viral skin infections. In particular, Staphylococcus aureus may exacerbate or maintain skin inflammation in atopic dermatitis by secreting a group of toxins known to act as superantigens .
|
|
Factors identified as being involved in the pathogenesis of atopic dermatitis include the differentiation of helper T cells, increased life span of eosinophils, multiple roles of IgE, the pattern of local cytokine expression, infectious agents, and superantigens .
|
|
The initiation of atopic dermatitis appears to be driven by allergen-induced activation of type 2 T-helper cells (Th-2 cells), leading to increased levels of IL-4, -10, and -13. Elevated IgE ensues. IgE contributes to the inflammatory cell infiltrate by several mechanisms, including immediate/late-phase reaction, allergen presentation by IgEbearing Langerhans cells, and allergen-induced activation of IgE-bearing macrophages.
The mononuclear cell infiltrate in the lesions probably reflects a combination of both IgE-dependent mast cell/ basophil degranulation and Th-2 cell-mediated responses elicited during acute exposure to allergens, including ingestants, inhalants, or contact aeroallergens such as human dander, grass pollens, and house dust mites .
|
|
The pattern of local cytokine expression plays an important role in modulating tissue inflammation and depends on the activity and/or duration of the lesion. Acute skin inflammation is associated with a predominance of IL-4 and IL13 expression, and little interferon-gamma (INF-y) But in chronic lesions, there are increased INF-y producing cells .
|
|
No specific single gene is a unique marker for atopic dermatitis. Genome screens of families with atopic dermatitis have implicated chromosomal regions that overlap with other skin diseases, including inflammatory and autoimmune skin disease . The dysfunctional skin barrier genes, which include loss of functional filaggrin , increase of protease activity, and lack of protease inhibitor, predispose the patients to the harmful effects of environmental agents . Chromosome 5q31 contains the IL-4 gene cluster family. Because IL-4 is central to the induction of IgE synthesis by B cells, it has been suggested that polymorphisms in the chromosome 5q31 region may be linked to the gene controlling total serum IgE in atopic individuals. Another possible candidate gene found on chromosome 11q13 is the high-affinity IgE receptor .
|
|

