|
Acanthosis nigricans =داء الشواك الأسود |
 |
 |
 |
|
Acanthosis Nigricans
Acanthosis nigricans can be seen in multiple clinical settings: malignancy associated, benign, inherited, obesity associated, syndromic, drug induced, and mixed (. The malignant
|
|
type differs from the benign types by showing more extensive and more pronounced lesions, by its progressiveness, and by its onset usually after 40 years of age. The histologic picture is essentially the same in all types.
|
|
The malignant type is associated with a malignant tumor-most commonly an abdominal, and particularly a gastric, carcinoma .However, it may also occur with squamous cell carcinoma, with sarcomas, and with Hodgkin and non-Hodgkin's lymphomas . In some cases, the skin lesions precede the symptoms of malignancy. The sign of Leser- Trelat, which is characterized by the sudden appearance of numerous seborrheic keratoses in association with a malignant tumor, may be an early stage or incomplete form of the malignant type of acanthosis nigricans. The seborrheic keratoses observed in this sign may be accompanied or followed by lesions of acanthosis nigricans
|
|
The benign inherited type usually has its onset during infancy or early childhood. It is an autosomal dominant trait .
|
|
Syndromic acanthosis nigricans is especially linked to syndromes associated with insulin resistance . In the HAIR-AN syndrome, which affects younger women, there is hyperandrogenemia (HA), insulin resistance (IR), and acanthosis nigricans (AN) (. Another subset links autoimmune states such as lupus erythematosus with uncontrolled diabetes mellitus, acanthosis nigricans, and ovarian hyperandrogenism. These patients have antibodies to the insulin receptor. Acanthosis nigricans has also been associated with insulin resistance in obesity, hypothyroidism, and congenital generalized lipodystrophy .
|
|
Acanthosis nigricans-like lesions have been induced by high dosages of nicotinic acid . Acanthosis nigricans has also occurred following use of oral contraceptives, following use of the folic acid antagonist triazinate, and as a localized reaction to insulin .
|
|
Clinically, acanthosis nigricans presents as papillomatous brown patches, predominantly in the intertriginous areas such as the axillae, the neck, and the genital and submammary regions (. In extensive cases of acanthosis nigricans of the malignant type, mucosal surfaces, such as the mouth, the vulva, and the palpebral conjunctivae, may be involved (29B). In the acral type, there is velvety hyperpigmentation of the dorsa of the hands and feet.
|
|
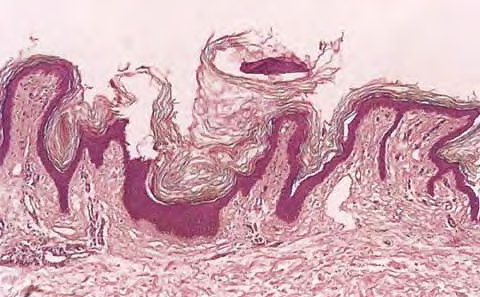
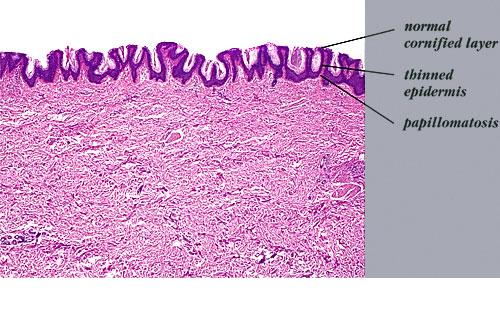
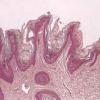
Histopathology.
Histologic examination reveals hyperkeratosis and papillomatosis but only slight, irregular acanthosis and usually no hyperpigmentation. Thus, the term acanthosis nigricans has little histologic justification.
|
|
In a typical lesion, the dermal papillae project upward as finger-like projections. The valleys between the papillae show mild to moderate acanthosis and are filled with keratotic material . Hom pseudocysts can occur in some cases . The epidermis at the tips of the papillae and often also on the sides of the protruding papillae appears thinned.
|
|
Slight hyperpigmentation of the basal layer is demonstrable with silver nitrate staining in some cases but not in others . The brown color of the lesions is caused more by hyperkeratosis than by melanin.
|
|
In the acanthosis nigricans lesions of the polycystic ovary syndrome, there are prominent deposits of
glycosaminoglycan consisting mostly of hyaluronic acid in the papillary dermis .
|
|
Histogenesis. The inherited type of acanthosis nigricans can be classified as a type of epidermal nevus. In persons who have acanthosis associated with insulin resistance, high levels of insulin may activate insulin-like growth factor-1 receptors and thereby mediate epidermal proliferation . Malignant acanthosis nigricans most likely is mediated by growth factors that are secreted by the associated neoplasm, such as transforming growth factoralpha . The basal cells from one patient with syndromic acanthosis nigricans demonstrated unusually high expression of the rare keratins 18 and 19 .
|
|
Differential Diagnosis
. Differentiation of acanthosis nigricans from other benign papillomas, particularly from linear epidermal nevi and from the hyperkeratotic type of seborrheic keratosis, may be difficult. As a rule, however, linear epidermal nevi show more marked acanthosis than acanthosis nigricans and have a more compact orthokeratotic stratum comeum. Furthermore, the pilosebaceous units in linear epidermal nevi are rudimentary. Acanthosis nigricans cannot be distinguished histologically from confluent and reticulated papillomatosis.
|
|
|
|
|