|
Porphyria
Seven types of porphyria are recognized . The light sensitivity in the six types with cutaneous lesions is caused by wavelengths that are absorbed by the porphyrin molecule. These wavelengths lie in the 400-nm range, representing long-wave ultraviolet light (UVA) and visible light .
|
|
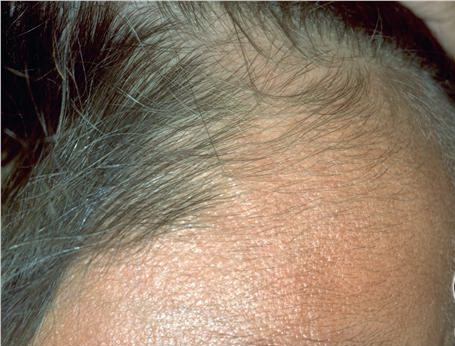
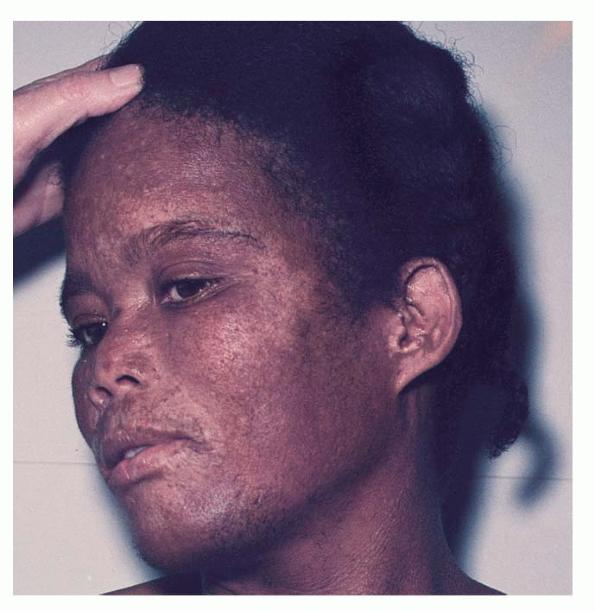
In erythropoietic porphyria, a very rare disease that typically develops during infancy or childhood, recurrent vesiculobullous eruptions in sun-exposed areas of the skin gradually result in mutilating ulcerations and scarring. It is inherited in an autosomal recessive pattern . Hypertrichosis and brown-stained teeth that fluoresce are additional features .
|
|
In erythropoietic protoporphyria, the usual reaction to light is erythema and edema followed by thickening and superficial scarring of the skin. In rare instances, vesicles are present that may resemble those seen in hydroa vacciniforme {93,94,95}. It is an autosomal dominant disorder that results from a mutation in the gene that codes for ferrochelatase, which is the final enzyme in the heme synthesis chain . The protoporphyrin is formed in reticulocytes in the bone marrow and is then carried in circulating erythrocytes and in the plasma. When a smear of blood from a patient is examined under a fluorescence microscope, large numbers of red-fluorescing erythrocytes are observed. The protoporphyrin is cleared from the plasma by the liver and excreted into the bile and feces {97}. It is not found in the urine. In rare instances, fatal liver disease develops quite suddenly, usually in persons of middle age {9B} but occasionally in patients only in the second decade of life .
|
|
In porphyria variegata, different members of the same family may have either cutaneous manifestations identical to those of porphyria cutanea tarda or systemic involvement analogous to acute intermittent porphyria, or both, or the condition may remain latent {95, 101}. The presence of protoporphyrin in the feces distinguishes porphyria variegata from porphyria cutanea tarda . Also, a sharp fluorescence emission peak at 626 nm is specific for the plasma of porphyria variegata {1 03,104}.
Three forms of porphyria cutanea tarda can be distinguished: sporadic, familial, and hepatoerythropoietic . In the sporadic form, only the hepatic activity of uroporphyrinogen decarboxylase is decreased. Almost all patients are adults, and no clinical evidence of porphyria cutanea tarda is found in other members of the patient's family. Although the sporadic form can occur without any precipitating factor, in most instances, in addition to the inherited enzymatic defect, an
|
|
acquired damaging factor to liver function is needed. The damaging agent most commonly is ethanol, but iron supplements, estrogen treatment, and hepatitis are also implicated {1 06, 1 07}.
In the familial form, a dominantly inherited disorder, in addition to the hepatic activity, the extrahepatic activity of uroporphyrinogen decarboxylase is decreased to about 50% of normal. The enzymatic activity usually is determined on the erythrocytes. The familial form may occur at any age, including childhood, and often, but not always, there is a family history of overt porphyria cutanea tarda. A reliable laboratory method for the diagnosis of the porphyrias is now provided by molecular genetics .
In the very rare hepatoerythropoietic form, the skin lesions appear in childhood and the activity of uroporphyrinogen decarboxylase in all organs is decreased to <10% of normal. Family studies suggest that these patients are homozygous for the gene that causes porphyria cutanea tarda {105}.
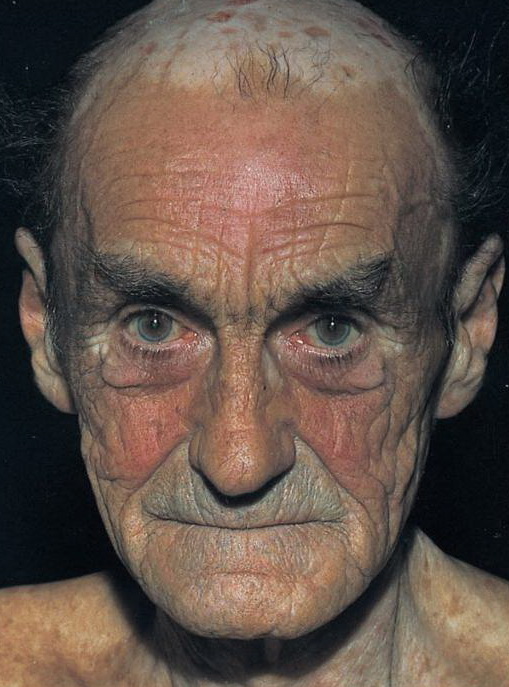
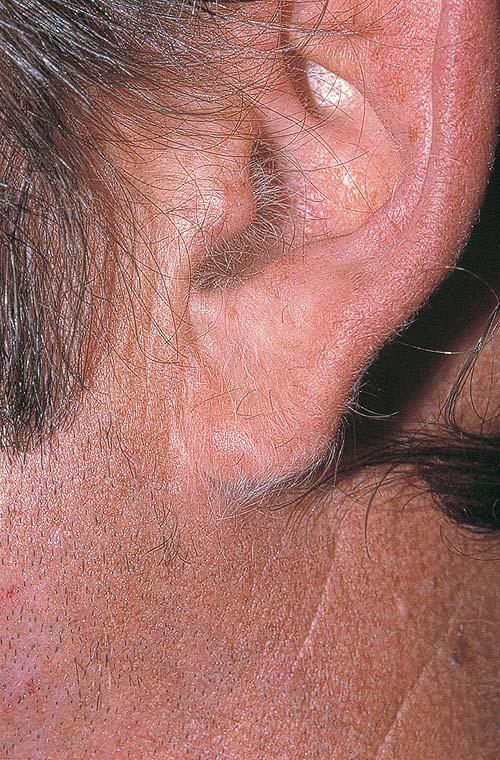
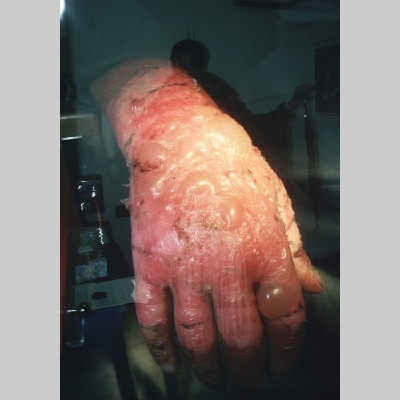
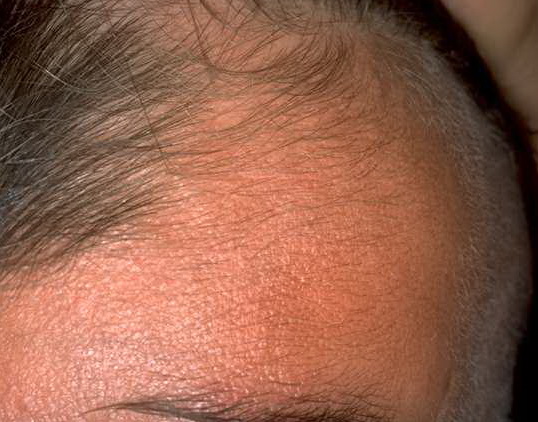
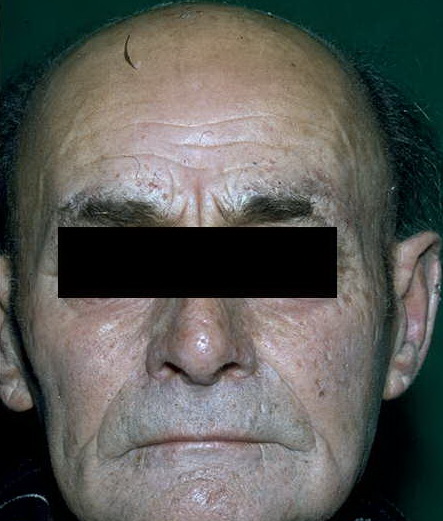
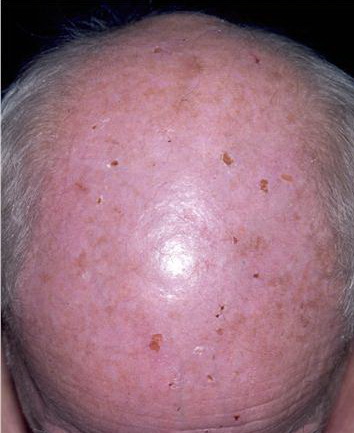
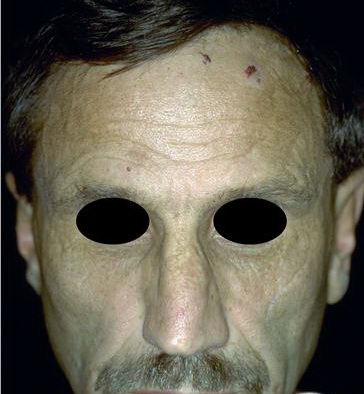
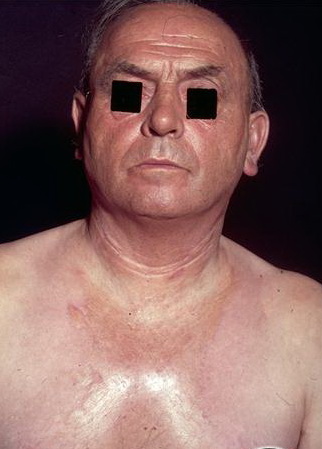
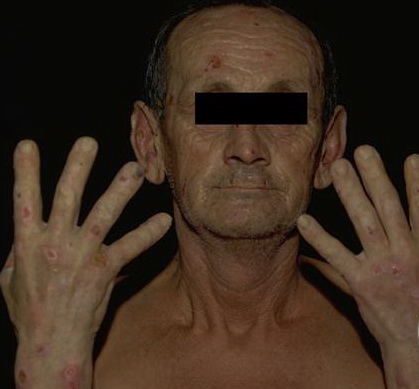
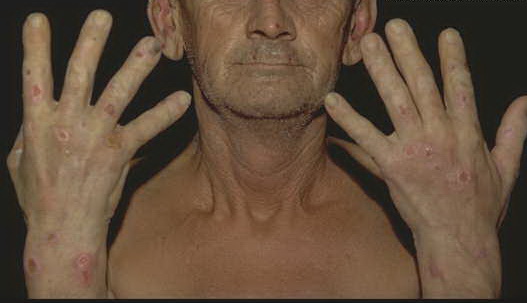
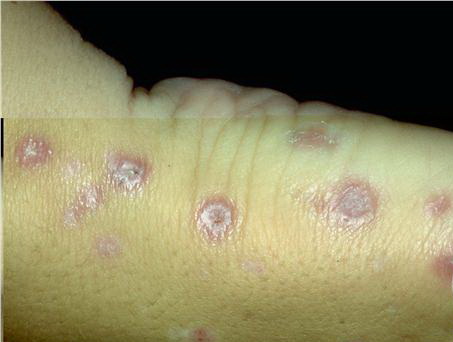
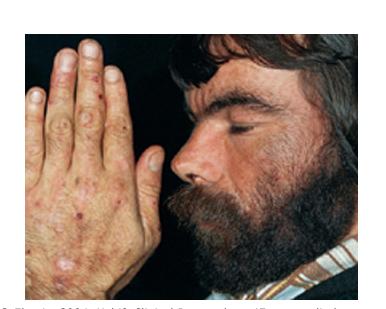
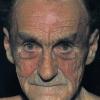
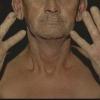
Clinically, the sporadic form of porphyria cutanea tarda, by far the most common type of porphyria, shows blisters that arise through a combination of sun exposure and minor trauma, mainly on the dorsa of the hands but sometimes also on the face {Fig. 17-9}. Mild scarring may result. The skin of the face and the dorsa of the hands often is thickened and sclerotic. Hypertrichosis of the face is common. Evidence of hepatic cirrhosis with siderosis is regularly present but generally is mild . In rare instances, hepatocellular carcinoma or a carcinoma metastatic to the liver induces porphyria cutanea tarda {109}. In the familial form of porphyria cutanea tarda, the clinical picture is similar to that of the sporadic form, but the changes are more pronounced. In the hepatoerythropoietic form, the manifestations are even more severe. On clinical grounds, the symptoms of most patients resemble those of erythropoietic porphyria, but when symptoms are milder, they resemble those of erythropoietic protoporphyria . Vesicular eruptions lead to ulceration, severe scarring, partial alopecia, and sclerosis {111}. Erythrocytes and teeth may show fluorescence . Liver damage develops with increasing age
|
|
In hereditary coproporphyria, a very rare disorder, there are episodic attacks of abdominal pain and a variety of neurologic and psychiatric disturbances analogous to those observed in acute intermittent porphyria and porphyria variegata . In some cases, there are also cutaneous manifestations indistinguishable from those of porphyria cutanea tarda and porphyria variegata .
|
|
Histopathology.
The histologic changes in the skin lesions are the same in all six types of porphyria with cutaneous lesions. Differences are based on the severity rather than on the type of porphyria. Homogeneous, eosinophilic material is regularly observed, and bullae are present in some instances. In addition, sclerosis of the collagen is present in old lesions .
|
|
In mild cases, homogeneous, pale, eosinophilic deposits are limited to the immediate vicinity of the blood vessels in the papillary dermis . These deposits are best visualized with a PAS stain, being PAS positive and diastase resistant.
|
|
In severely involved areas, which are most common in erythropoietic protoporphyria, the perivascular mantles of homogeneous material are wide enough in the papillary dermis to coalesce with those of adjoining capillaries. In addition, deeper blood vessels may show homogeneous material around them, and similar homogeneous material may be found occasionally around eccrine glands . PAS staining demonstrates this material particularly well. In some instances, it also contains acid mucopolysaccharides, shown with Alcian blue or the colloidal iron stain , or lipids, demonstrable with Sudan IV or Sudan black B . In addition, the PAS-positive dermalepidermal basement membrane zone may be thickened .
|
|
In areas of sclerosis, which occur especially in porphyria cutanea tarda, the collagen bundles are thickened. In contrast to scleroderma, PAS-positive, diastase-resistant material is often present in the dermis in perivascular locations .
|
|
The bullae, which are most common in porphyria cutanea tarda and least common in erythropoietic protoporphyria, arise subepidermally . Some blisters are dermolytic and arise beneath the PAS-positive basement membrane zone ; others form in the lamina lucida and are situated above the PAS-positive basement membrane zone . It has been suggested thatthe blisters in porphyria cutanea tarda in mild cases arise within the junctional zone but that in severe cases they form beneath the PAS-positive basement membrane zone and thus heal with scarring . It is quite characteristic of the bullae of porphyria cutanea tarda that the
|
|
dermal papillae often extend irregularly from the floor of the bulla into the bulla cavity (104,122). This phenomenon, referred to as festooning, is explained by the rigidity of the upper dermis induced by the presence of eosinophilic material within and around the capillary walls in the papillae and the papillary dermis.
|
|
The epidermis forming the roof of the blister often contains eosinophilic bodies that are elongate and sometimes segmented (123). These "caterpillar bodies" are PAS positive and diastase resistant. Ultrastructurally, they have been found to contain three components: (a) cellular organelles, including melanosomes, desmosomes, and mitochondria; (b) colloid that may be located intracellularly or extracellularly; and (c) electron-dense material thought to be of basement membrane origin (124).
|
|
On electron microscopic examination, concentric duplications of the basement membrane around the dermal blood vessels are observed. Peripheral to this multilayered basement membrane, one observes a thick mantle of unlayered material with the same filamentous and amorphous composition as that of the basement membrane. Often, a gradual transition from the layered to the unlayered zone can be observed . Scattered through the thick, unlayered zone are solitary collagen fibrils with an average diameter of only 35 nm, in contrast to the 100 nm of mature collagen . In cases with severe involvement, intermingled filamentous and amorphous material is seen throughout the upper dermis and even in the mid dermis.
|
|
Proof that the perivascular material in porphyria represents excessively synthesized basement membrane material and as such contains type IV collagen is provided by positive immunofluorescence staining with anti-type IV collagen monospecific antibody . The presence of small collagen fibrils analogous to reticulum fibrils suggests the presence also of type III collagen.
|
|
In the majority of patients, direct immunofluorescence testing has revealed the presence of immunoglobulins, particularly immunoglobulin G (lgG) , and occasionally also of complement (128), in the walls of blood vessels and at the dermal-epidermal junction of light-exposed skin. It is unlikely that these deposits indicate an immunologic phenomenon; rather, they are the result of "trapping" of immunoglobulins and complement in the filamentous material.
|
|
The enzymatic defect that causes each form of porphyria is known . Enzyme determinations may be carried out on cultured skin fibroblasts, erythrocytes, or liver tissue.
|
|
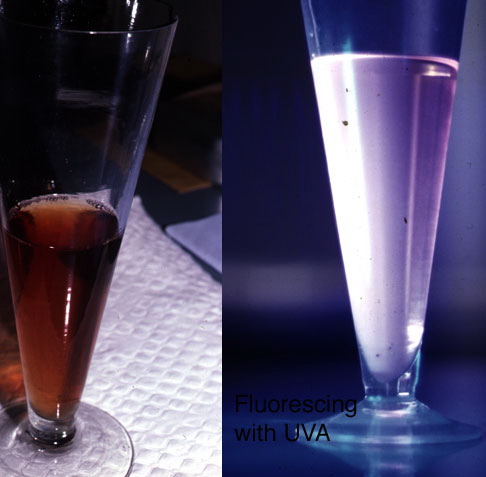
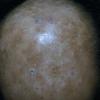
Liver damage is generally mild and chronic in porphyria cutanea tarda. In erythropoietic protoporphyria, however, liver function tests are usually normal, even though microscopic deposits of protoporphyrin in the liver are found frequently . Yet, in rare instances, death occurs from liver failure developing swiftly after the initial detection of hepatic dysfunction . Patients with liver failure have very high levels of protoporphyrin in the erythrocytes and at the time of death show extensive deposits of protoporphyrin in a cirrhotic liver. The protoporphyrin in hepatocytes and Kupffer cells appears as dark brown granules . This pigment exhibits birefringence on polariscopic examination and in unstained sections viewed with ultraviolet light shows red autofluorescence . In patients with normal liver function tests, biopsy of the liver mayor may not show portal and periportal fibrosis .
|
|
Pseudoporphyria Cutanea Tarda
In patients with chronic renal failure who are receiving maintenance hemodialysis, an eruption indistinguishable from that of porphyria cutanea tarda may develop on the dorsa of the hands and fingers during the summer months . Rarely, blisters are seen also on the face, and atrophic scarring develops . In a series of 180 patients receiving hemodialysis, 28 (16%) showed this type of eruption . Normal porphyrin levels in urine, stool, and plasma are the rule in hemodialyzed patients developing clinical signs of porphyria cutanea tarda. However, in a few patients receiving hemodialysis for chronic renal failure, a true porphyria cutanea tarda coexists . In such patients, if a certain degree of diuresis persists, urinalysis may not be representative of the porphyria metabolism, and the plasma and fecal porphyrins should always be measured .
|
|
Pseudoporphyria cutanea tarda may also occur following the ingestion of certain drugs, such as furosemide, nalidixic acid, tetracycline hydrochloride, and naproxen (135). Because many patients on hemodialysis for renal failure also are receiving furosemide, withdrawal of the drug can determine whether the dialysis or the medication is the cause of the pseudoporphyria, because in drug-induced cases, withdrawal of the drug is curative .
|
|
Histopathology. In patients with pseudoporphyria, the histologic picture is indistinguishable from that seen in mild cases of porphyria. The superficial blood vessels show thickened walls, and the PAS-positive basement membrane zone is often thickened as well. Blisters are subepidermal, with festooned dermal papillae. The blisters usually are situated above the PAS-positive basement membrane zone .
|
|
immunoglobulins are often observed in vessel walls and at the dermal-epidermal junction. Complement is also occasionally present .
|
|