Geographic Tongue
Geographic tongue (benign migratory glossitis) is a benign condition that occurs in up to 3% of the general population. Most often, patients are asymptomatic; however, some patients report increased sensitivity to hot and spicy foods. The etiology and pathogenesis of geographic tongue are still poorly understood. Geographic tongue affects males and females and is noted to be more prominent in adults than in children.1,2
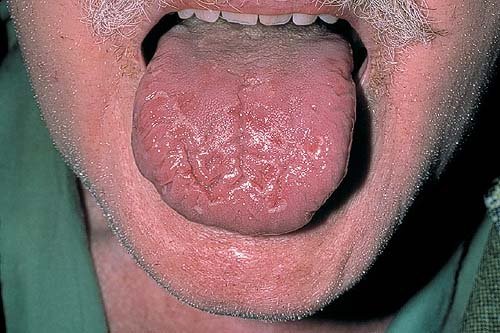
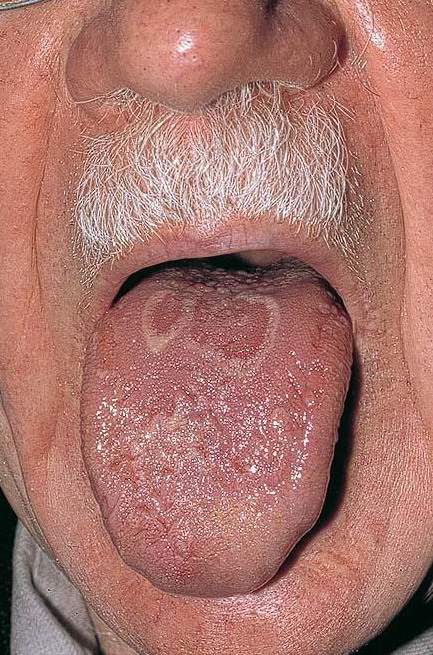
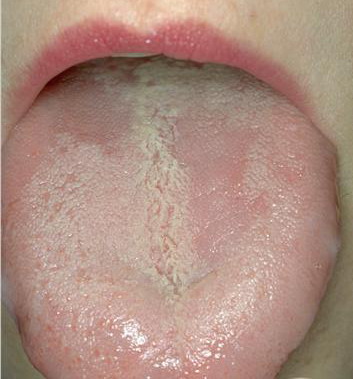
The classic manifestation of geographic tongue is an area of erythema, with atrophy of the filiform papillae of the tongue, surrounded by a serpiginous, white, hyperkeratotic border. The patient often reports spontaneous resolution of the lesion in one area, with the return of normal tongue architecture, only to have another lesion appear in a different location of the tongue. Lesion activity in geographic tongue may wax and wane over time, and patients are occasionally free of lesions. If lesions occur at other mucosal sites, the condition is termed erythema migrans.
The most commonly affected site is the tongue; however, other oral mucosal soft tissue sites may be affected. Geographic tongue has been reported with increased frequency in patients with psoriasis3,4,5,6,7 and in patients with fissured tongue.8,9 Although geographic tongue is an inflammatory condition histologically, a polygenic mode of inheritance has been suggested because it is seen clustering in families. Associations with human leukocyte antigen (HLA)–DR5, HLA-DRW6, and HLA-Cw6 have also been reported.10,11
Geographic tongue has reportedly occurred in up to 3% of the general population in the United States.
International frequency rates for geographic tongue are similar to those reported in the United States.
Geographic tongue is a benign condition.
No racial or ethnic predilection is reported for geographic tongue.
Females have been reported to be affected twice as often as males.12 Exacerbations have been suggested to be related to hormonal factors.
Geographic tongue can affect all age groups; however, it is more predominant in adults than in children.
- Patients with geographic tongue may present with a burning sensation or an irritation of the tongue noted with hot or spicy foods.
- Patients may report that the discomfort waxes and wanes over time, and they routinely describe that the lesions affect different areas of the tongue at different times.
- Patients are occasionally concerned about the diagnosis of oral cancer, which prompts them to be evaluated, despite reporting that they have noted these lesions over many years.
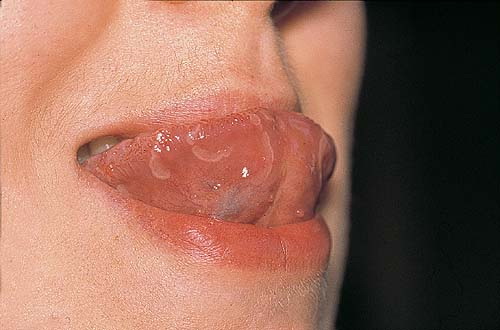
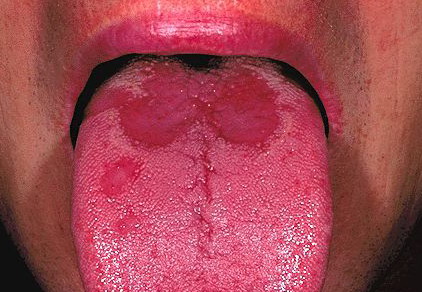
- The tongue exhibits a well-demarcated area of erythema, primarily affecting the dorsum, and often extending to involve the lateral borders of the tongue.
- Within the area of erythema, the normal tongue architecture is effaced, with loss of the filiform papillae and atrophy of the overlying mucosa.
- Surrounding this area of erythema is a well-defined, hyperkeratotic, yellow-white border with an irregular serpiginous outline.
- Similar lesions may be present concurrently on other aspects of the tongue or other mucosal sites, including the floor of the mouth and cheek the mucosa.13
- A definitive cause has not been elucidated, but lesions are seen with increased frequency in patients with psoriasis. In a study of patients with psoriasis, geographic tongue occurred in 10% of the patients, in contrast to only 2.5% of age- and sex-matched controls.14
- A polygenic mode of inheritance has been suggested for geographic tongue.15
No increased incidence of geographic tongue has been noted with medication use or environmental agents
Treatment
No medical intervention is required because the lesion is benign and most often asymptomatic. However, Abe et al report successful treatment with cyclosporin,17 and Sigal and Mock reported treatment with topical and systemic antihistamines.18
Consultation with an oral pathologist is indicated if a question exists about the diagnosis.