Hirsutism
EPIDEMIOLOGY
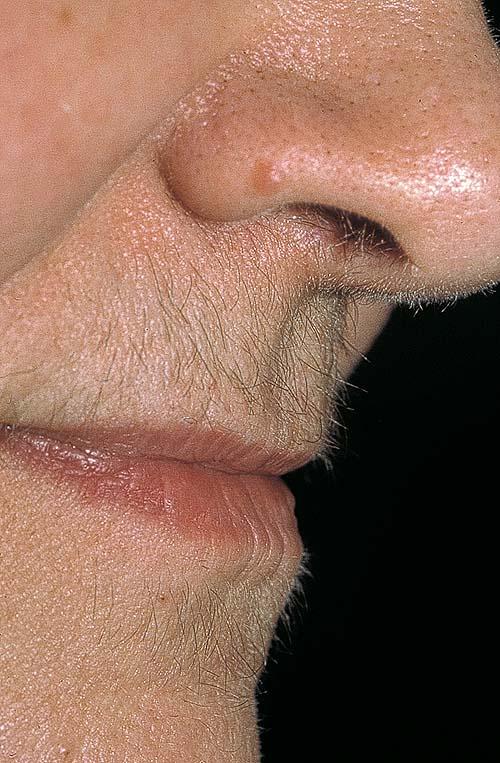
What constitutes significant hirsutism is difficult to define, as it depends on a variety of cultural and racial factors, media-driven perceptions of normality, and the perceptions of the individual physician and patient. Not surprisingly, therefore, estimates of the frequency of hirsutism in the female populations have varied widely. In London, 1.2 percent of women were significantly hirsute. Other studies have reported frequencies of up to 18 percent. The frequency and distribution of female androgen-dependent hair growth also varies with age; terminal hair growth in the pubic and axillary regions declines with age, whereas facial hair growth increases. These difficulties have led to the use of the patient-determined term unwanted hair to influence therapeutic decision making. Nevertheless, the physician may still have to make a value judgment as to when patient concerns really represent a body dysmorphic disorder, rather than a problem solvable by hair removal.
PATHOGENESIS
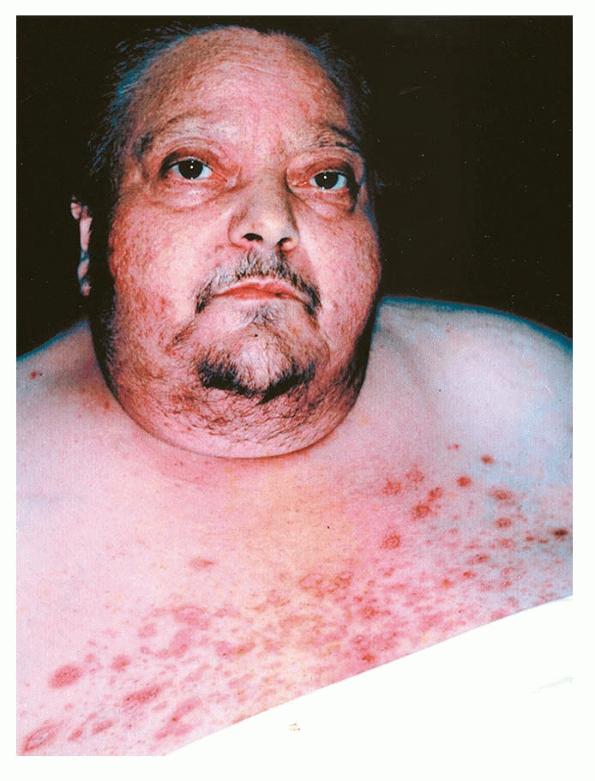
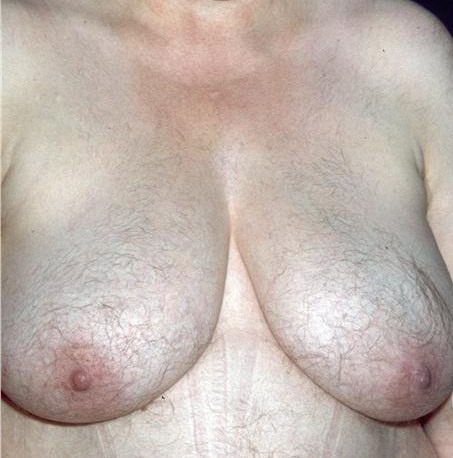
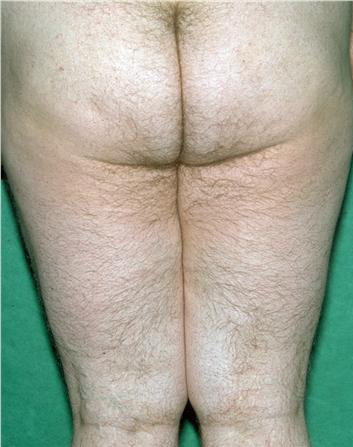
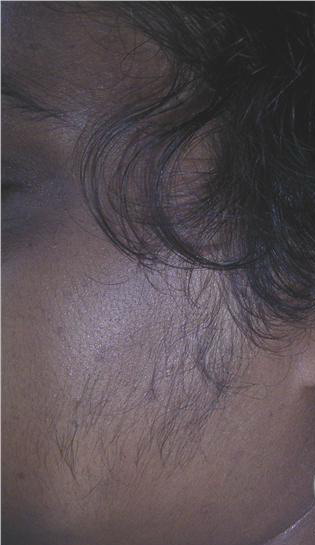
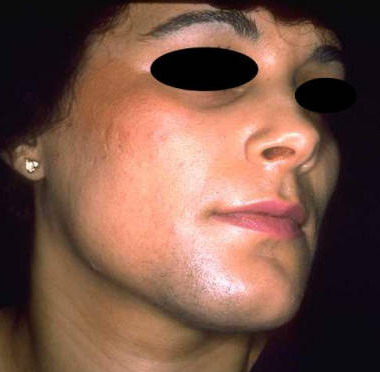
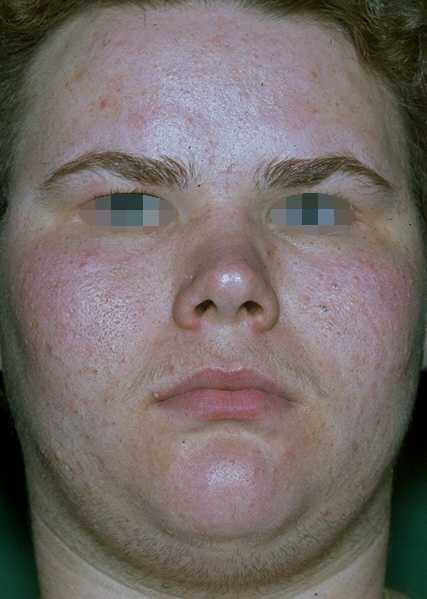
Terminal hair growth in a “male” pattern is undoubtedly due to the effect of androgens, and reflects the conversion of vellus to terminal hair follicles. In many women, hirsutism is associated with raised levels of circulating androgens (54 percent in one series). However, in some, androgen levels are within the normal range, suggesting in these individuals that hair growth is especially sensitive to androgen stimulation. Recent evidence suggests that testosterone increases 5α-reductase gene expression in dermal papillae from lower abdominal skin of women with hirsutism; theoretically, this may raise the dihydrotestosterone-generating potency of these hair follicles.302 Also, only certain 5α-reductase type 1 haplotypes are reportedly associated with hirsutism, which further raises the question of whether inherited, constitutive abnormalities in intrafollicular dihydrotestosterone synthesis are an important element in the pathogenesis of hirsutism. Other clinical features of hyperandrogenism include oligo- or amenorrhea, sub- or infertility, acne, acanthosis nigricans, and female pattern hair loss to frank virilization with male pattern balding and clitoromegaly. Table 86-8 lists causes of hyperandrogenism, of which polycystic ovary syndrome is by far the most common.
INVESTIGATION
Whether and how to investigate hirsute women depends on a number of factors, including the presence of clinical features of increased androgen production, the duration of the history, and the concerns of the patient. In fertile women with normal menses and a long history of relatively mild hirsutism, it is debatable whether investigation is necessary at all. In women with moderate to severe hirsutism, particularly when accompanied by other signs of androgen excess, further evaluation is warranted (. Women with hyperprolactinemia may have an increase in functional androgens through adrenal overproduction and through a decrease in sex hormone-binding globulin caused by a diminution of ovarian estrogen production.
|
|
|
•
|
Androgen-secreting tumors
|
|
|
•
|
Adrenal
|
|
|
|
•
|
Adenoma
|
|
|
|
•
|
Adenocarcinoma (rare)
|
|
|
|
•
|
Ectopic adrenocorticotropic hormone-secreting tumor (rare)
|
|
|
•
|
Ovarian
|
|
|
|
•
|
Gonadal stromal tumor
|
|
|
|
•
|
Thecoma
|
|
|
|
•
|
Lipoid tumor
|
|
Functional androgen excess
|
|
|
•
|
Adrenal enzyme deficiencies (congenital adrenal hyperplasia)
|
|
|
|
•
|
Early onset 21-hydroxylase deficiency
|
|
|
|
•
|
Late-onset 21-hydropxylase deficiency
|
|
|
|
•
|
11β-hydroxylase deficiency
|
|
|
|
•
|
3β-ol dehydrogenase deficiency
|
|
|
•
|
Cushing syndrome
|
|
|
•
|
Polycystic ovarian disease
|
|
|
|
•
|
With or without adrenal contribution
|
|
|
|
•
|
Hyperthecosis
|
|
•
|
“Idiopathic” hirsutism
|
|
•
|
Medication/drug use
|
|
Hughes CL: Hirsutism, in Disorders of Hair Growth: Diagnosis and Treatment, edited by Olsen EA. New York, McGraw-Hill, 1994, p 344, Table 14-2.
|
|
TREATMENT
The approach is two-pronged: the removal or reduction of existing unwanted terminal hair, and the reduction of the androgen drive toward further vellus-terminal transformation. The latter approach (e.g., using anti-androgens) may also help to reduce hair growth but, on its own, is unlikely to eliminate it . Shaving, plucking, and use of depilatory creams are temporary means of hair removal that can be irritating and painful. The topically applied inhibitor of ornithine decarboxylase, eflornithine 13.9 percent, is approved for the reduction of unwanted facial hair in women when applied twice daily.
Recommended Investigation for Hirsutism
|
- Serum testosterone (if > 200 ng/mL, exclude androgen-secreting tumor)
- Serum-free testosterone and dehydroepiandrosterone (more sensitive; most women with moderately elevated androgen levels have polycystic ovarian syndrome)
- 17-hydroxyprogesterone (raised level suggests congenital adrenal hyperplasia; confirm diagnosis by repeat measurement after adrenocorticotropic hormone stimulation)
- Serum prolactin (hyperprolactinemia due to macro- or microprolactinoma or treatment with neuroleptic drugs331; may have associated menstrual abnormalities, infertility, and galactorrhea)
|
|
Box 86-3 Treatment of Hirsutism
Remove existing terminal hair and prevent further vellus-to-terminal transformation
- Temporary hair removal
- Shaving, plucking, depilatory creams
- Topical eflornithine (slows growth; does not remove hair)
- (Potentially) permanent hair removal
- Electroepilation
- Laser hair removal
- Anti-androgen measures
- Weight loss
- Oral anti-androgens (spironolactone, cyproterone acetate)
- Oral contraceptives
- Finasteride
Laser epilation is less permanent than often suspected, is most effective when applied repetitively, and patients should be discouraged from unrealistic expectations. The mechanism of laser epilation is the selective photothermolysis of melanized hair through absorption of light energy. The combination of the topically applied eflornithine with laser therapy may decrease the growth after hair removal.
Weight loss may be helpful in obese patients because obesity increases free testosterone levels by reducing sex hormone-binding hormone and contributes to insulin resistance.
There are marginal differences in efficacy between systemically administered agents, but all generally take 6 to 12 months for sufficient miniaturization of terminal hairs to be clinically significant. These include oral anti-androgens (such as spironolactone, 100 to 200 mg daily) or cyproterone acetate, oral contraceptives, and finasteride. Oral contraceptives inhibit androgen synthesis by inhibiting the output of gonadotropins and are most effective if combined with anti-androgens. Treatment of congenital adrenal hyperplasia may also be accomplished
through the use of low-dose dexamethasone. Hyperprolactinemia may be treated directly with either medical (bromocriptine) or surgical treatment of the hyperprolactinoma, possibly combined with an anti-androgen.