
















































Erythema Nodosum
Erythema nodosum is the most common type of septal panniculitis. It is not a disease but a reaction pattern to a variety
of etiologic agents . It may occur at any age, but most cases appear between the second and fourth decades of life. It is much more common in women than in men. The eruption
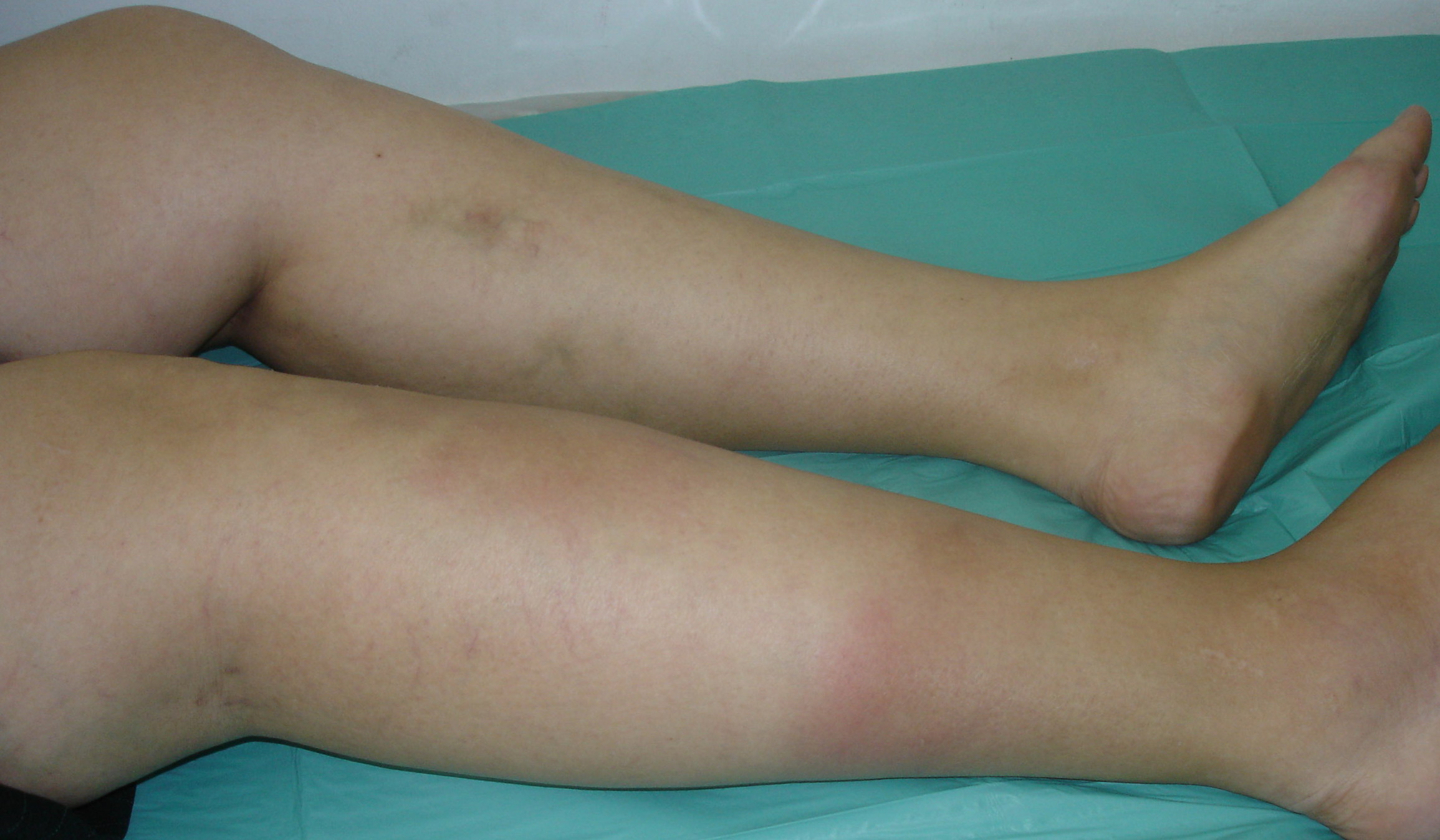
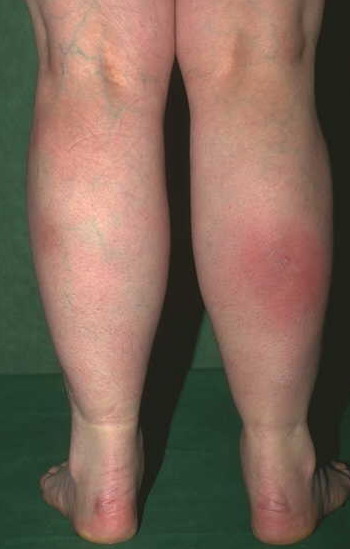
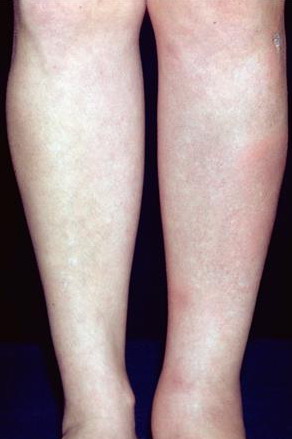
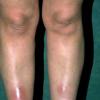
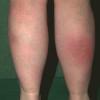
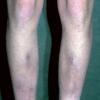
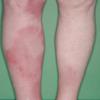
consists of a sudden onset of symmetric, tender, erythematous, warm nodules and raised plaques with bilateral distribution, usually on the anterior aspect of the lower extremities . Within a few days, the nodules show a vivid red or purplish color that evolves to a yellow or greenish coloration, which resembles a deep bruise, the so-called erythema contusiforme. Ulceration is never seen in erythema nodosum, and the lesions heal without atrophy or scarring. Acute bouts of erythema nodosum are associated with a fever, fatigue, malaise, arthralgia, headache, abdominal pain, vomiting, cough, or diarrhea. The eruption generally lasts from 3 to 6 weeks, and recurrences are frequent.
ERYTHEMA NODOSUM AT A GLANCE
Clinical
- · Symmetric, tender, erythematous, warm nodules and raised plaques on the anterior aspects of the lower extremities
- · Acute onset
- · No ulceration
- · More common in women than in men
Histopathology
- · Mostly septal panniculitis without vasculitis
- · Thickened septa with inflammatory cells
- · Neutrophils in early lesions and histiocytes and Miescher granulomas in late-stage lesions
Treatment
|
Etiologic Factors in Erythema Nodosum
|
|
Infections
|
Drugs
|
|
|
• Bacterial infections
|
|
• Sulfonamides81
|
|
|
|
• Streptococcal infections50
|
|
• Bromides82
|
|
|
|
• Tuberculosis51
|
|
• Iodides82
|
|
|
|
• Yersinia infections52
|
|
• Oral contraceptives83
|
|
|
|
• Salmonella infections53
|
|
• Minocycline84
|
|
|
|
• Campylobacter infections54
|
|
• Gold salts85
|
|
|
|
• Brucellosis55
|
|
• Penicillin86
|
|
|
|
• Tularemia56
|
|
• Salicylates86
|
|
|
|
• Atypical mycobacterial infections57
|
|
• Chlorothiazides71
|
|
|
|
• Chancroid57
|
|
• Phenytoin71
|
|
|
|
• Meningococcemia57
|
|
• Aminopyrine57
|
|
|
|
• Corynebacterium diphtheriae infections57
|
|
• Arsphenamine57
|
|
|
|
• Cat-scratch disease58
|
|
• Hepatitis B vaccine86
|
|
|
|
• Propionibacterium acnes59
|
|
• Nitrofurantoin57
|
|
|
|
• Shigella infections60
|
|
• Pyritinol61
|
|
|
|
• Gonorrhea61
|
|
• D-penicillamine87
|
|
|
|
• Syphilis62
|
|
• Thalidomide88
|
|
|
|
• Leptospirosis63
|
|
• Isotretinoin89
|
|
|
|
• Q fever64
|
|
• Interleukin 290
|
|
|
|
• Lymphogranuloma venereum65
|
Malignant Diseases
|
|
|
|
• Chlamydia psittaci infections66
|
|
• Hodgkin disease91
|
|
|
|
• Mycoplasma pneumoniae infections67
|
|
• Non-Hodgkin lymphoma92
|
|
|
• Viral infections
|
|
• Leukemia93
|
|
|
|
• Infectious mononucleosis68
|
|
• Sarcoma61
|
|
|
|
• Hepatitis B69
|
|
• Renal carcinoma90
|
|
|
|
• Milker's nodules70
|
|
• Post-radiotherapy for pelvic carcinoma94
|
|
|
|
• Orf71
|
Miscellaneous Conditions
|
|
|
|
• Herpes simplex57
|
|
• Sarcoidosis95
|
|
|
|
• Measles71
|
|
• Ulcerative colitis96
|
|
|
|
• Cytomegalovirus infections72
|
|
• Colon diverticulosis61
|
|
|
• Fungal infections
|
|
• Crohn disease97
|
|
|
|
• Dermatophytes73
|
|
• Behçet disease98
|
|
|
|
• Blastomycosis74
|
|
• Reiter syndrome99
|
|
|
|
• Histoplasmosis75
|
|
• Sweet syndrome100
|
|
|
|
• Coccidioidomycosis76
|
|
• Pregnancy101
|
|
|
|
• Sporotrichosis57
|
|
• Takayasu arteritis102
|
|
|
|
• Aspergillosis77
|
|
• Immunoglobulin A nephropathy103
|
|
|
• Protozoal infections
|
|
• Chronic active hepatitis104
|
|
|
|
• Toxoplasmosis78
|
|
• Granulomatous mastitis105
|
|
|
|
• Ancylostomiasis57
|
|
• Vogt-Koyanagi disease106
|
|
|
|
• Amebiasis79
|
|
• Sjögren syndrome106
|
|
|
|
• Giardiasis79
|
|
|
|
|
|
• Ascariasis80
|
|
|
|
The classically described processes of erythema nodosum migrans,43-46 subacute nodular migratory panniculitis of Vilanova and Piñol, and chronic erythema nodosum,49 are now just considered clinical variants of erythema nodosum.
The list of etiologic factors associated with erythema nodosum is very long, including infectious diseases, medications, malignancies, and a wide group of miscellaneous conditions (see Table 68-1).50-106 Although there are considerable geographic variations related to endemic infections, streptococcal infections are the most frequent etiologic factor of erythema nodosum in children. In contrast, drugs, sarcoidosis, and inflammatory bowel disease are the most commonly associated disorders in adults with erythema nodosum. Erythema nodosum is considered to be a hypersensitivity response to a large number of inciting factors.
Erythema nodosum is the stereotypical histologic example of a mostly septal panniculitis with no vasculitis. The connective tissue septa of the subcutis appear thickened with inflammatory cells that extend to the periseptal areas of the fat lobules . As in other panniculitides, the composition of the inflammatory infiltrate in the septa of erythema nodosum lesions varies with age of the lesion, with neutrophils being the predominant cells in early lesions, whereas histiocytes and small granulomas are seen in late-stage lesions. A characteristic histopathologic marker of erythema nodosum is the so-called Miescher radial granuloma, which consists of small, round, well-defined nodular aggregations of small histiocytes radially arranged around a minute slit The nature of the central cleft is unknown, and immunohistochemical and ultrastructural studies have failed to demonstrate endothelial or other cellular lining of these clefts. In older nodules of erythema nodosum, histiocytes coalesce to form multinucleated giant cells , many of which still keep in their cytoplasm a stellate central cleft reminiscent of those centers of Miescher radial granuloma. Another histopathologic characteristic of erythema nodosum is the absence of vasculitis.110 In late-stage lesions of erythema nodosum, the septa are markedly widened with granulation tissue at the interface between septa and fat lobules. With time, the lesions resolve without atrophy or scarring of the involved septa.
Treatment of erythema nodosum should be directed toward the associated disorder. Usually, nodules of erythema nodosum regress spontaneously within a few weeks, and bed rest is often sufficient treatment. Aspirin, nonsteroidal anti-inflammatory drugs and 2 to 10 drops of a saturated solution of potassium iodide may be helpful to enhance analgesia and resolution.111-116 Systemic corticosteroids are rarely indicated in erythema nodosum, and an underlying infection should be ruled out before these drugs are administered.