| Erythema chronicum migrans=الحمامى المزمنة الهاجرة |
|
|
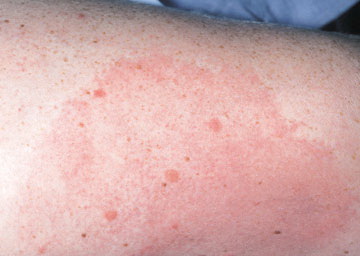
Erythema chronicum migrans
Lyme disease is a systemic infection caused by the spirochete Borrelia burgdorferi.1 The bacteria are inoculated into the skin by a tick bite, nearly always from hard-bodied ticks of the genus Ixodes. The original descriptions of the dermatologic manifestations of Lyme disease date back to 1883 in Europe, when a German physician, Alfred Buchwald, described what is now termed acrodermatitis chronica atrophicans (ACA). Several decades later in 1912, a Swedish dermatologist, Arvid Afzelius, described erythema chronicum migrans (ECM), which currently is referred to simply as erythema migrans (EM).
It was not until 1975, when a statistically improbable cluster of childhood arthritis occurred in and around the town of Lyme, Connecticut, that the full spectrum of the disease began to be elucidated. This outbreak stimulated intense clinical and epidemiologic research that led to the discovery of the causative agent and its ecology and an expanding geographic range and list of clinical manifestations. In addition, the initial antibiotic responsiveness of the cutaneous manifestations that had been described in the 1950s in the European literature was confirmed, and the findings were extended. In 1998, the US Food and Drug Administration (FDA) approved a protective vaccine, but the manufacturer pulled it from the market a few years later.
PathophysiologyThe pathophysiology of Lyme disease is incompletely understood. Many of its manifestations are caused by active infection by the spirochete; others may be driven by immunopathogenetic mechanisms. While any part of the body can be affected, the organism shows a distinct tropism for the skin, heart, central nervous system (CNS), joints, and eyes. The bacteria are introduced into the skin by a bite from an infected Ixodes tick. In the northeastern and upper midwestern United States, Ixodes scapularis (sometimes termed Ixodes dammini) is the vector. In the northwestern United States, Ixodes pacificus is the vector. In other parts of the world, other Ixodes ticks serve this function. Other tick species (eg, Amblyomma americanum) and insects can carry B burgdorferi, but the vast majority of cases are believed to be caused by bites by Ixodes ticks. Note that in the southern and midcentral United States, a Lyme-like disease has been reported for which the vector appears to be A americanum. Patients with erythema migrans from Missouri and those from New York have different clinical and microbiological aspects of the disease. B burgdorferi has not been isolated from the southern patients, although a closely related spirochete is suspected to be involved. Although some cases from the southern United States are documented with this new spirochete, called Borrelia lonestari, no organism can be isolated in the vast majority of cases of erythema migrans in this geographical area.2,3 Once in the skin, the spirochete can be overwhelmed and eliminated by host defense mechanisms, can remain viable but localized at the site of inoculation, or may disseminate via blood and lymphatics. Hematogenous dissemination can occur within days or weeks of the initial infection. The organism can travel to other parts of the skin, the heart, joints, the CNS, and other parts of the body. Early studies showed that in roughly 10% of patients with isolated erythema migrans and no systemic symptoms, B burgdorferi or its DNA, can be detected in the bloodstream. In addition, early in the course of disease and while erythema migrans still is present, spirochetal DNA has been detected in cerebrospinal fluid, indicating early CNS penetration. This can occur even in the absence of neurologic symptoms. Importantly, one 2005 study found that if large-volume cultures (9 mL of plasma) were performed in early presenting patients with erythema migrans, 93 (43.7%) of 213 had spirochetemia. Some of these patients had only isolated erythema migrans and no systemic symptoms.4 The organism also can persist in the skin for very long periods of time. Experimentally, the spirochete can penetrate human fibroblasts and live intracellularly, even when the extracellular medium contains ceftriaxone at concentrations well above bacteriocidal levels. While intracellular organisms have never been demonstrated in vivo, this may be one mechanism by which the organism eludes host defense mechanisms. Clinically, B burgdorferi has been cultured from skin lesions of patients with acrodermatitis chronica atrophicans 10 years after initial infection. Because people who engage in activities that put them in risk for tick bites tend to continue those activities, reinfection is not uncommon. Patients who have had prior erythema migrans can be reinfected (meaning that the first infection has been successfully treated and they have a new infection with B burgdorferi). This has been clearly demonstrated in reinfected patients who were culture positive and had different serotypes isolated in the first and second infections. Reinfection shows similar manifestations as first infections, although a tendency towards less hematogenous spread is noted. In contrast, relapse (as opposed to reinfection) is very unusual in patients who have been treated with appropriate antimicrobials.5
Note that while many patients present with erythema migrans, others first present with extracutaneous symptoms, either because erythema migrans never occurred or because it was not recognized by the patient or correctly diagnosed by the physician. The last important phenomenon to appreciate is co-infection by other organisms transmitted by the same tick bite. Co-infection by ehrlichial species and Babesia microti are reported with increased frequency; in some studies, in as many as 10-15% of patients with Lyme disease. When Lyme disease is strongly suggested but some of the manifestations are atypical, these other tick-borne infections must be considered.
HistoryEpidemiologic context is extremely important. Since only approximately 25-30% of patients with early Lyme disease recall the tick bite, the history must be directed by the clinician towards the possibility of a tick bite. Determining where the patient lives, works, and vacations is important, as is asking about specific activities in which the patient participates at those locales. The likelihood of Lyme disease increases as the probability of a tick bite increases in a geographically endemic area. Systemic manifestations are as follows:
PhysicalIn many patients with early Lyme disease, physical examination alone is sufficient to establish the diagnosis of erythema migrans. Careful attention to the details often makes the difference between the need to proceed with further confirmatory tests and an empiric course of antibiotics. In particular, the examination must be interpreted in the epidemiologic context; this cannot be overemphasized. The season, geography, and a patient's activities in those areas can be important diagnostic clues A low-grade fever is not uncommon. High fever suggests another co-infecting tick-borne organism such as Ehrlichia or Babesia species or some other diagnosis altogether such as streptococcal cellulitis.
Rashes very similar to erythema migrans have been reported in the southern United States from which B burgdorferi cannot be cultured. This disease is called southern tick-associated rash illness (STARI), or Master disease. As a group, distinctions can be made between classic erythema migrans and this illness, but significant overlaps exist such that the differences are not useful in diagnosing individual patients. A number of important details are diagnostically useful. Note the following:
Regional lymphadenopathy may be seen. Borrelial lymphocytoma usually occur on the earlobe or nipple, and the lesions are bluish-red nodules. The earlobe is the typical location in children (as is the scrotum), while the nipple location is more commonly seen in adults. Borrelial lymphocytoma tends to occur in areas of prior (or concurrent erythema migrans). The size is up to a few centimeters. Regional lymphadenopathy may be present (see the image below). Borrelial lymphocytoma is a form of B-cell pseudolymphoma. Other terms used to describe borrelial lymphocytoma include lymphadenosis benigna cutis, lymphocytoma cutis, cutaneous lymphoid hyperplasia, and Spiegler-Fendt lymphoid hyperplasia. Acrodermatitis chronica atrophicans begins as an inflammatory phase marked by edema and erythema, usually on the distal extremities. At times, a faint bluish discoloration is found predominantly on extensor surfaces. The lesions have a predilection for the posterior heels and dorsal (extensor) surfaces of the hands, feet, elbows, and knees. Gradually, a central progression of the area involved occurs over months to years. The lesions also tend to become symmetric. The buttocks often become involved. Later, atrophy supervenes and thin cigarette-paper skin is seen. Because of the loss of subcutaneous fat, underlying venous structures are more visible, and the skin becomes thin, atrophic, and dry. Fibrous juxtaarticular nodules or bands may be seen on the extensor surfaces of the elbows and knees. Signs of peripheral neuropathy may coexist with acrodermatitis chronica atrophicans.
CausesThe cause of Lyme disease is infection by the spirochete, B burgdorferi. This organism, whose complete genome was described in 1998, has several distinct genetic groupings; as well, there is evidence that additional strains or closely related Borrelia species also exist.
The primary risk factor for developing cutaneous manifestations of Lyme disease is exposure to Ixodes ticks.
Laboratory StudiesIn most patients with erythema migrans (EM), a carefully elicited history (including definitions of epidemiologic context) and a physical examination are all that is required to establish the diagnosis. The US Centers for Disease Control and Prevention (CDC) accepts physician-diagnosed erythema migrans of greater than 5 cm in size in its case definition. (In clinical practice, erythema migrans can be smaller than this size. The 5-cm limit was designed for surveillance purposes.) No tests, including serologic tests for Lyme disease, are indicated in these patients. CBC counts and erythrocyte sedimentation rates often are normal. Antibody titers B burgdorferi may be falsely negative at this early stage of disease and should not affect the decision to treat.
Most, but not all, patients with borrelial lymphocytoma are seropositive for antiborrelial antibodies. This is true for all early disseminated manifestations of Lyme disease.
Histologic FindingsHistologic findings in erythema migrans are nonspecific, usually showing a perivascular cellular infiltrate consisting of lymphocytes, plasma cells, and histiocytes. Occasionally, mast cells and neutrophils are seen. Central biopsies may show eosinophilic infiltrate consistent with a local reaction to an arthropod bite. Spirochetes occasionally may be identified using silver or antibody-labeled stains, although usually, a paucity of spirochetes is found in the tissues of patients with Lyme disease. In addition, cultures for B burgdorferi are positive in approximately 75% of patients. In acrodermatitis chronica atrophicans, biopsy specimens from early lesions show a lymphocytic dermal infiltrate, sometimes perivascular in location, with some vascular telangiectasia and lymphedema. Plasma cells also may be seen in the cellular infiltrate. Later lesions demonstrate epidermal thinning with loss of skin appendages. At this stage, plasma cells may be the only feature to distinguish acrodermatitis chronica atrophicans from morphea. The fibrotic nodules show fibrosis of the deeper dermis and sometimes, hyalinization of collagen bundles. B burgdorferi occasionally can be cultivated from the lesions; in 1 patient, cultivation was successful more than 10 years after the lesion's first appearance
Medical CareCutaneous manifestations of Lyme disease are treated using antibiotics. Important considerations include the stage of the disease, presence of associated neurologic symptoms or signs (especially in borrelial lymphocytoma [BL] and acrodermatitis chronica atrophicans [ACA]), and patient factors (duration of symptoms, allergies, age, pregnancy status). Controversies in treatment and diagnostic entities Controversy regarding the treatment of Lyme disease abounds, including an antitrust investigation by the Connecticut Attorney General into the development process for the Lyme disease treatment guidelines from the Infectious Disease Society of America. The Attorney General claimed the process was tainted by suppression of scientific evidence and conflicts of interest.12 Controversy also surrounds many aspects of the diagnosis and treatment of Lyme disease. Some have proposed existence of an "Axis of Evil," which would include the Internet, for promoting Lyme hysteria; particular specialty laboratories, for allegedly performing inaccurate testing; and physicians, specifically those who prescribe prolonged and unnecessary courses of antibiotic treatment.13 The existence and treatment of conditions termed chronic Lyme disease and posttreatment Lyme disease have been called into question as a result of a lack of direct evidence of persistent infection.14,15 Extended antibiotic therapy, sometimes longer than 6 months, has been advocated for these poorly defined conditions, which not only can cause great harm to patients but has resulted one or more deaths.16 Hassett et al report associated psychiatric comorbidity in patients with chronic Lyme disease.17 In 2006, the guidelines committee of the Infectious Disease Society of America stated that a group of symptoms termed "persistent Lyme disease symptoms" (eg, headaches, mood disturbances, fatigue, poor memory, joint pain) are merely the "aches and pains of daily living." Further, an ad hoc international Lyme group stated they are "symptoms common in persons who have never had Lyme disease." Cameron has proposed that despite the controversy surrounding persistent Lyme disease symptoms, evidence to deny care is lacking and to do so is neglectful to patient care.
MedicationIn general, skin manifestations of Lyme disease respond promptly to appropriate antibiotic therapy. Early manifestations respond more rapidly than later manifestations. Data regarding the best route and duration of antibiotic therapy are evolving and are, to some extent, controversial. Some researchers claim an abundance of overtreatment and overdiagnosis of Lyme disease, pointing to several nonspecific conditions and symptoms that have been linked to Lyme disease. They indicate that if these sequelae remain after appropriate therapy, other causes must be carefully and conclusively excluded.20 For solitary erythema migrans, oral antibiotics clearly provide effective therapy. The duration of recommended therapy ranges from 10-30 days. In the past, this author has recommended 3 weeks of treatment, since a sizable minority of patients with solitary erythema migrans have evidence of hematogenous dissemination, even in the absence of symptoms. In addition, strong evidence indicates that patients with early disseminated Lyme disease have equally good outcomes after 3 weeks of oral antibiotics compared with 2 weeks of parenteral therapy. Therefore, patients with erythema migrans and asymptomatic disseminated disease are treated adequately using the 3-week course. Borrelial lymphocytoma usually is treated with 14-21 days of oral antibiotics, but when symptoms of dissemination are noted, parenteral therapy sometimes is used. Borrelial lymphocytoma is sufficiently uncommon that no comparative trials address the ideal duration of treatment, route of administration of the antibiotic, or the choice of medication. For the same reasons as in erythema migrans, some logic exists in using a 3-week course of antibiotics. Acrodermatitis chronica atrophicans usually is treated with 1-month course of oral antibiotics, usually a beta-lactam or doxycycline. One study showed fewer relapses with 30 days compared to 20 or fewer days of therapy. In the same study, 30 days of oral antibiotics were more effective than 15 days of IV ceftriaxone (2 g/d).23 Ensure that no neurologic manifestations are present before embarking on oral therapy. AntibioticsDirected against B burgdorferi sensu lato. They are indicated for all the cutaneous manifestations of Lyme disease. Amoxicillin (Amoxil, Dispermox, Trimox)DOC for pediatric patients <9 y and may be used in pregnancy (assuming parenteral antibiotics are not used). Does not treat disease from co-infecting organisms (eg, ehrlichiosis, babesiosis). Adult250-500 mg PO tid; not to exceed 3 g/d Pediatric20-50 mg/kg/d PO divided tid; not to exceed 3 g/d Probenecid (Benemid) increases effects Documented hypersensitivity PregnancyB - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals PrecautionsAdjust dose in renal impairment Doxycycline (Vibramycin)DOC for adults with erythema migrans. Inhibits protein synthesis and, thus, bacterial growth by binding to 30S and possibly 50S ribosomal subunits of susceptible bacteria. Advantage is that it covers co-infecting ehrlichial and rickettsial species. Adult100 mg PO bid Pediatric<8 years: Not recommended Bioavailability decreases with antacids containing aluminum, calcium, magnesium, iron, or bismuth subsalicylate; tetracyclines can increase hypoprothrombinemic effects of anticoagulants. PregnancyD - Fetal risk shown in humans; use only if benefits outweigh risk to fetus PrecautionsPhotosensitivity may occur with prolonged exposure to sunlight or tanning equipment; reduce dose in renal impairment; consider drug serum level determinations in prolonged therapy; tetracycline use during tooth development (last one half of pregnancy through age 8 y) can cause permanent discoloration of teeth; Fanconilike syndrome may occur with outdated tetracyclines Cefuroxime (Ceftin)Second-generation cephalosporin maintains the gram-positive activity of first-generation cephalosporins. Has explicit FDA approval for erythema migrans. For cost reasons, it is an alternate drug. Adult500 mg PO bid PediatricChildren: 250 mg PO bid for 20 d Disulfiram-like reactions may occur when alcohol is consumed within 72 h after taking cefuroxime; may increase hypoprothrombinemic effects of anticoagulants; may increase nephrotoxicity in patients receiving potent diuretics such as loop diuretics; coadministration with aminoglycosides increases nephrotoxic potential Documented hypersensitivity PregnancyC - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus PrecautionsAdminister one-half dose if CrCl level is 10-30 mL/min and one-quarter dose if <10 mL/min (high doses may cause CNS toxicity); bacterial or fungal overgrowth of nonsusceptible organisms may occur with prolonged or repeated therapy Erythromycin (E-Mycin, Eryc, Ery-Tab)Inhibits bacterial growth, possibly by blocking dissociation of peptidyl tRNA from ribosomes arresting RNA-dependent protein synthesis. For treatment of staphylococcal and streptococcal infections. Adult 250 mg erythromycin stearate/base (or 400 mg ethylsuccinate) PO q6h, or 500 mg q12h (1 h ac or 2 pc) Pediatric30-50 mg/kg/d (15-25 mg/lb/d) PO divided q6-8h; double dose for severe infection Coadministration may increase toxicity of theophylline, digoxin, carbamazepine, and cyclosporine; may potentiate anticoagulant effects of warfarin; coadministration with lovastatin and simvastatin increases risk of rhabdomyolysis Documented hypersensitivity; hepatic impairment PregnancyB - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals PrecautionsCaution in liver disease; estolate formulation may cause cholestatic jaundice; GI tract adverse effects are common (administer doses pc); discontinue if nausea, vomiting, malaise, abdominal colic, or fever occur Azithromycin (Zithromax)Second-line drug. Like erythromycin, has excellent in vitro sensitivities but has underperformed compared to amoxicillin in 1 large study. Conversely, in several European studies, has been shown to be equal to beta-lactam and tetracycline group antibiotics. Because of once-daily dosing, should be considered in pregnant patients who are allergic to beta-lactams and in patients where compliance is a major issue. Adult500 mg PO qd for 5 d, followed by 5-day hiatus, then second course of 500 mg PO qd for 5 d Pediatric10 mg/kg PO once on day 1; not to exceed 500 mg/d, followed by 5 mg/kg PO on days 2-5; not to exceed 250 mg/d May increase toxicity of theophylline, warfarin, and digoxin; effects are reduced with coadministration of aluminum and/or magnesium antacids; nephrotoxicity and neurotoxicity may occur when coadministered with cyclosporine Documented hypersensitivity; hepatic impairment; do not administer with pimozide PregnancyB - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals PrecautionsSite reactions can occur with IV route; bacterial or fungal overgrowth may result with prolonged antibiotic use; may increase hepatic enzymes and cholestatic jaundice; caution in patients with impaired hepatic function, prolonged QT intervals, or pneumonia; caution in patients who are hospitalized, geriatric, or debilitated |