



YAWS (FRAMBOESIA TROPICA, PIAN, BUBA, PARU, PARANGI)
Epidemiology and Etiology
Yaws is caused by T. pallidum (subspecies pertenue). The spirochete can be propagated in laboratory animals, and various strains have been isolated for investigation. Approximately 75 percent of new cases arise in children younger than 15 years of age. Yaws is contracted from direct contact with abraded, bitten, or excoriated skin with oozing lesions. Some experts contend, with scant evidence, that the disease can be transmitted by flies or through domestic utensils.7
Differential Diagnosis of Pinta
Most Likely
- · Leukodermas
- · Eczema (early lesions)
Consider
- · Pityriasis alba
- · Pellagra
- · Tinea versicolor
- · Melasma
- · Lichen planus (early lesions)
- · Tuberculoid leprosy (early lesions)
- · Tinea corporis
- · Psoriasis (early lesions)
- · Lupus erythematosus (early lesions)
- · Yaws (early lesions)
- · Syphilis
Always Rule Out
- · Vitiligo
- · Erythema dyschromicum perstans
The infection occurs in countries along the tropical belt in lowlands characterized by heavy rainfall, high humidity, and persistently hot temperatures above 27°C (80.6°F). Owing to mass treatment campaigns and improved living conditions, the disease has been eradicated in many areas, and greatly reduced in others.5 However, yaws is underdiagnosed because fewer physicians have experience with the infection. Over the past three decades, due to relaxed surveillance and control measures and the persistence of poor sanitary conditions, a resurgence of yaws has been documented in regions of Africa and Southeast Asia. Sizable foci have been reported in several tropical regions of western and central Africa (Ghana, Togo, Benin, and the Central African Republic), and residual foci remain in South America (Colombia, Guyana, Peru, Ecuador, and Brazil), Haiti, Dominica, Southeast Asia, Indonesia, Papua New Guinea, and the Solomon Islands.7 Currently, at least 100 million children are estimated to be at risk of becoming infected.1 T. pallidum pertenue is nearly identical to the spirochete that causes infectious and endemic syphilis, so not surprisingly the diseases share many characteristics.
Primary Stage
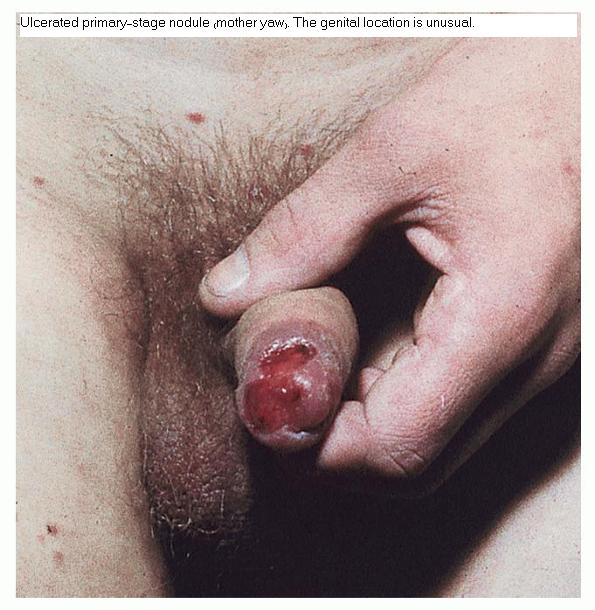
After an incubation period of 10 to 90 days (average, 3 weeks), the primary lesion or mother yaw (buba madre) appears at the site of inoculation, which is usually an exposed body part, generally a lower extremity.8 Characteristically, the lesion is a non-tender, often pruritic, infiltrated, erythematous small nodule that grows to a size of 1 to 5 cm. Its surface frequently becomes papillomatous and crusted. The primary lesion is usually single, but satellite papules may be present, becoming confluent into a plaque. The lesion eventually becomes an ulcer (chancre of yaws, frambesioma) with a raspberry-like base that may be covered by yellow crust . Regional buboes (enlarged lymph nodes) are common.The mother yaw heals spontaneously in 2 to 6 months, leaving atrophic scarring and central hypopigmentation. Constitutional symptoms are rare.
Secondary Stage
Resolution of the mother yaw is typically followed by a period of latency, which is then interrupted within 10 to 16 weeks, but possibly as long as 2 years, after the onset of the primary stage by an eruption of disseminated skin lesions with generalized lymphadenopathy. Constitutional symptoms such as malaise, fever, and anorexia are often present. The lesions (daughter yaws or pianomas) are reddish, weeping, warty or vegetating, crusted, non-pruritic papules and plaques that are similar to but smaller than (up to 2 cm) the mother yaw . As the lesions grow, they become eroded and covered by a highly infectious fibrinous exudate, which dries into a crust . The exudate attracts flies that torture the affected persons. Pianic onychia (paronychia) may develop.
Pianomas may appear in any body area. In addition, dry, papulosquamous patches and plaques (pianides) may be present on any part of the body.8 In body folds (axillae, anal folds), they are
resemble condylomata lata; on mucous membranes, they are similar to hypertrophic mucous patches. It is interesting that widespread warty exudative lesions appear during humid times, but in arid, desert regions and during dry spells, the lesions favor or are limited to intertriginous areas and mucous membranes. In addition, a milder, attenuated, less florid form with small, dry, few (even single) lesions that are often limited to skin folds has been reported in areas with low or receding transmission rates. In some cases the lesions are papillomatous but resolve quickly.
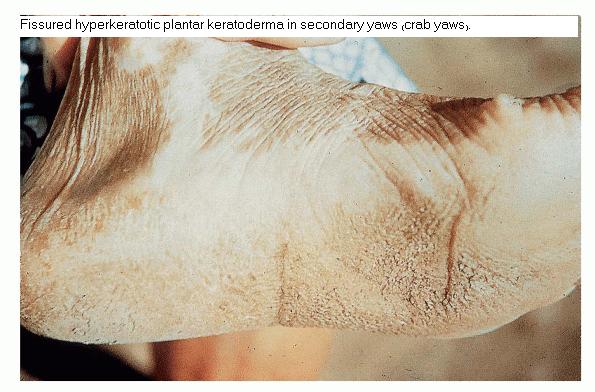
Thick, hyperkeratotic plaques of the palms and soles become fissured and ulcerated (“worm-eaten soles”). This painful involvement of the soles is also called crab yaws because patients walk with a deliberate slow, crustacean gait. Lesions may be annular or circinate (tinea yaws). Lesions on the face are often seborrheic or psoriasiform.8 Painful osteoperiostitis is common in early yaws.7 The appearance of turnip-like, fusiform soft-tissue swelling of the proximal, but not the distal, phalanges because of periostitis is classic (“ghoul hands”). The metatarsal, metacarpal, and tibial bones are also commonly involved. Infected persons then enter a latent period with serologic reactivity but no signs or symptoms of the disease. All lesions resolve without scarring, but relapses may develop during the initial 5 years of infection. In relapsing yaws, lesions tend to be confined to the perioral, perianal, and periaxillary areas.
Tertiary Stage
In approximately 10 percent of cases, latency is interrupted after 5 to 10 years by a late stage with skin and skeletal lesions, and possibly with ophthalmologic and neurologic involvement. Cutaneous
and subcutaneous gummatous nodules (gumma framboesiodes) necrose centrally and ulcerate, causing deep, mutilating lesions. Coalescence of the ulcers may produce circinate, serpiginous tracts that heal with deforming scars and contractures.6 Palmoplantar hyperkeratosis may lead to chronic keratoderma. Juxta-articular lymphadenopathy may occur on the elbows and knees.
Late skeletal changes include hypertrophic periostitis, hydrarthrosis, gummatous osteitis and periostitis, and osteomyelitis. Considerable bone hypertrophy as a result of chronic osteitis may result in curvature of the tibia (saber shins). Bilateral hypertrophic osteitis of the nasal process of the maxillae with persistent swelling of the nasal bridge (goundou) slowly progresses over 5 to 20 years. The most dreaded consequence of yaws, which occurs in approximately 1 percent of untreated infected persons, is rhinopharyngitis mutilans (gangosa), or extensive destruction of the nose, maxillae, upper lip, and central face with eventual perforation of the nose and palate. Although ophthalmologic, neurologic, and cardiovascular disease is not usually associated with yaws, there are rare reports of optic disk atrophy, myeloneuropathy, and aneurysms.
Differential Diagnosis
Differential Diagnosis of Yaws
Most Likely
- · Frambesiform leishmaniasis (pianomas, gangosa)
- · Paracoccidiomycosis (pianomas)
Consider
- · Psoriasis (pianides)
- · Impetiginized eczema (pianides)
- · Pyoderma vegetans (pianomas)
- · Arthropod bites (pianides)
- · Myiasis (pianides)
- · Scabies (pianides)
- · Dermatophytosis (pianides)
- · Pyoderma (pianomas)
- · Lupus vulgaris (gangosa)
- · Atypical mycobacterial infection
- · Deep fungus infection (pianotes, gangosa)
- · Tuberculoid leprosy (pianides)
- · Ecthyma (pianomas)
- · Vitiligo (pintoids)
- · Pinta (pintoids)
- · Keratodermas
Always Rule Out
- · Frambesiform syphilis (pianides, pianomas)