| Blastomycosis= الفطار البرعمي |
|
|
Blastomycosis
Blastomycosis, which originally was described by Gilchrist and Stokes in 1894 and 1896, is an infection with a highly variable spectrum of clinical presentations. Disease can range from an asymptomatic, self-healing pulmonary infection to widely disseminated fatal disease. Blastomyces dermatitidis is a dimorphic fungus. The mycelial form grows as a white mold. The conidia (spores) that convert to yeast are infectious to humans. The epidemiology is incompletely understood because of the lack of a sensitive and specific skin test and difficulties in establishing the ecologic niche of the organism in nature. In the United States, most infections are clustered in states adjacent to the Mississippi and Ohio rivers and the Great Lakes region. Although initial epidemiologic studies reported a higher incidence of infection in men, more recent series have shown no predilection for any specific sex, age, race, or occupation or any seasonal variation. The disease is uncommon in children but is now recognized increasingly in immunocompromised hosts, particularly in patients with acquired immune deficiency syndrome (AIDS).1 Infection is acquired via inhalation of the conidia. Once in the lungs, the conidia need to mature into invasive yeast for infection to occur. Immunocompetent hosts have a natural resistance to infection with Blastomyces because alveolar macrophages inhibit the transformation of conidia into yeast. Such natural resistance is supported by studies of blastomycosis epidemics, in which asymptomatic infection occurs in at least 50% of persons in whom Blastomyces has colonized. The factors that determine whether disease develops in infected persons are unclear. Cellular immune host resistance has been difficult to evaluate for its role in protection against infection but is probably an important factor for asymptomatic versus overt infection.
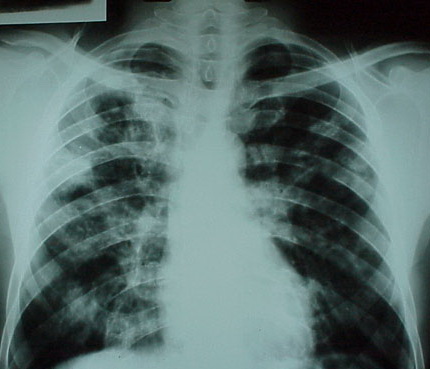
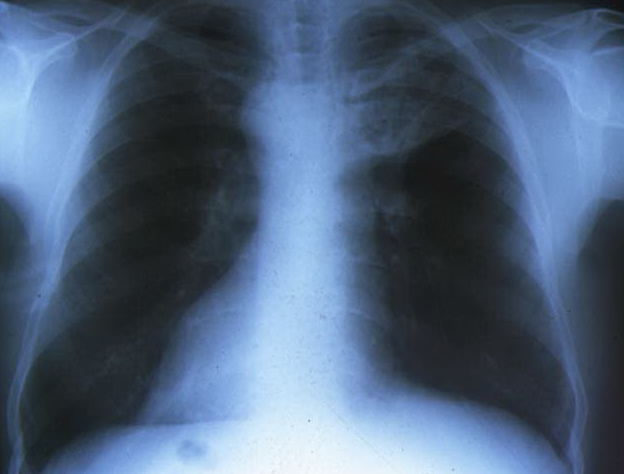
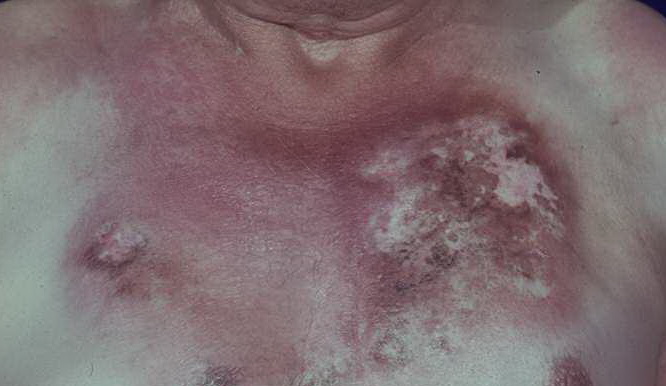
PathophysiologyThe term B dermatitidis refers to the imperfect (asexual) stage of Ajellomyces dermatitidis, which grows as a yeast at 37°C and mycelial form at room temperature. Two serotypes of B dermatitidis have been detected by exoantigen analysis. The perfect (ie, sexual form), A dermatitidis, is heterothallic and requires 2 compatible mating types for spore formation. The mycelial form, which bears conidiophores, produce single terminal conidia, which measure 2-10 µm in diameter and are round or oval. Primary infection, which may be subclinical, occurs in the lung following inhalation of fungal conidia. Transition from the mold form to the yeast form occurs after deposition in the distal airways. The phase shift occurs as a result of heat-related stress, followed by uncoupling of oxidative phosphorylation. In the absence of nonspecific host defense mechanisms, cells increase in number in the lung parenchyma. Hilar lymph nodes may become involved, and, subsequently, lymphohematogenous spread to the other organs may occur. Incubation time averages 4-6 weeks and widely varies. Subclinical cases of blastomycosis occur in at least 50% of infected individuals, thus supporting the hypothesis that some patients have natural resistance. Cellular immune response mediated by antigen-specific T lymphocytes and lymphokine-derived macrophage's cell-mediated immunity plays a critical role in aborting fungal growth The clinical spectrum of blastomycosis widely varies, including asymptomatic infection (in nearly one half of patients infected), acute or chronic pneumonia, and extrapulmonary disease.
Physical
CausesB dermatitidis is a thermal dimorphic fungus that occurs in mycelial form in nature and as yeast in infected tissue.
Laboratory StudiesThe following studies are indicated in patients with blastomycosis:
Imaging Studies
Other Tests
Procedures
Histologic Findings
Medical Care
Surgical Care
MedicationAmphotericin B remains the antifungal agent with the most success against B dermatitidis. Cumulative doses less than 1 g have resulted in cure without relapse in 70-91% of adult cases of blastomycosis. A retrospective study of blastomycosis cases in Mississippi reported a cure rate of 86.5% and a relapse rate of only 3.9% for patients treated with amphotericin.10 Toxicity often necessitates interruption of therapy. Cutaneous and noncavitary lung disease should be treated for approximately 8-10 weeks. Cavitary lung disease or infection that extends beyond the lung and skin should be treated for about 10-12 weeks with a cumulative dose of 2.5 g or more of amphotericin B. Amphotericin B is the drug of choice for treating children with life-threatening and central nervous system infections caused by blastomycosis. Most experts recommend a total cumulative dose of 30 mg/kg or higher of amphotericin B. Human trials of lipid formulations of amphotericin B in the treatment of blastomycosis have not been performed. However, limited clinical data suggest that these preparations may be used for selected patients intolerant to standard amphotericin B therapy. The azoles are an equally effective and less toxic alternative to amphotericin B for treating adult immunocompetent patients with mild-to-moderate pulmonary or extrapulmonary disease, excluding CNS disease. In a multicenter clinical trial involving adult patients, itraconazole was found to be more effective and associated with fewer adverse effects than ketoconazole.7 Most experts recommend a minimum of 6 months of oral azole therapy for mild-to-moderate pulmonary or nonmeningeal disseminated blastomycosis. Safety and efficacy data using oral azole therapy in children are limited. Itraconazole has been used successfully as treatment in a small number of pediatric patients with non–life-threatening non-CNS disease. Short courses of amphotericin B (5-10 mg/kg total dose) followed by oral itraconazole for 6 months may be used to treat extrapulmonary blastomycosis. The oral azoles are not beneficial in treating CNS blastomycosis. If oral azole antifungal agents are used for non–life-threatening cases, patients should be closely monitored. Amphotericin B should be substituted for the oral azole agent if clinical deterioration is noted or serum levels of medications are not adequate. Acute pneumonia complicated by acute respiratory distress syndrome and extrapulmonary disease may need treatment with moderate doses of amphotericin B (>1.5 g total dose) or short courses of amphotericin B (500 mg total dose) followed by 6 months of oral itraconazole. In pregnant women with blastomycosis, amphotericin B is the drug of choice because the oral azoles are contraindicated due to their embryotoxic and teratogenic effects. Although unusual, in recent years, an increased number of cases of blastomycosis have been reported in compromised hosts, including patients with AIDS, bone marrow and solid organ transplant recipients, and patients receiving cytotoxic or long-term immunosuppressive therapy. Early and aggressive therapy with amphotericin B therapy is warranted because multiple organ and CNS involvement with resultant mortality is relatively common in this population. Furthermore, response to antifungal therapy may be suboptimal, and relapses are common. Most experts recommend treating blastomycosis in children with AIDS with 30 mg/kg of amphotericin B over 4-6 weeks, followed by itraconazole for at least 6 months in those who have responded to a primary course of amphotericin B. Until more data are available, primary therapy with itraconazole should be used with caution in compromised patients with blastomycosis and considered only in mild illness without CNS infection and stable or improving disease. Long-term suppressive therapy may be needed in immunocompromised patients. Some experts recommend itraconazole as probably the best secondary prophylaxis for AIDS patients with blastomycosis. Antifungal agentsTheir mechanism of action may involve an alteration of RNA and DNA metabolism or an intracellular accumulation of peroxide that is toxic to the fungal cell. Amphotericin B (Amphocin, Fungizone)Initial DOC for blastomycosis in patients with severe illness (eg, rapidly progressive infections, CNS disease), immunocompromised hosts, and special circumstances (eg, pregnancy, childhood disease). Adult0.7-1 mg/kg/d IV; total cumulative dose 1.5-2.5 g; CNS disease warrants at least 2 g total dose PediatricAdminister as in adults; total cumulative dose >30 mg/kg IV Nephrotoxic drugs may cause additive toxic effects; corticosteroids may increase potassium depletion caused by amphotericin; may predispose patients receiving cardiac glycosides or skeletal muscle relaxants to toxicity secondary to hypokalemia Documented hypersensitivity; renal failure limits the use of amphotericin B PregnancyB - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals PrecautionsBecause of the nephrotoxic potential of amphotericin, other nephrotoxic drugs should be avoided; administered by IV infusion over 2-6 h at a final concentration not to exceed 0.1 mg/mL; monitoring parameters include electrolyte levels, BUN levels, serum creatinine levels, and CBC count; regularly; monitor input and output; monitor for signs of hypokalemia (eg, muscle weakness, cramping, drowsiness, ECG changes) Itraconazole (Sporanox)PO itraconazole (at a dosage of 200-400 mg/d) is now the azole of choice in adult patients with indolent nonmeningeal blastomycosis of mild-to-moderate severity, whether given as primary therapy to stable patients or following a course of amphotericin B. Compared with other PO azoles, itraconazole is better absorbed and has enhanced antimycotic activity with fewer adverse effects. In a prospective phase 2 clinical trial involving adult patients, itraconazole was effective in 90% of cases receiving 200-400 mg/d. In a cohort study of 42 patients, similar success rates were noted for patients treated with 200 mg of itraconazole. Adult200-400 mg/d PO with food (to enhance absorption); 200 mg/d initially; if poor response, increase dose in 100 mg increments; not to exceed 400 mg/d in 2 divided doses Pediatric5-7 mg/kg/d PO qd or divided q12h Decreased effect of itraconazole with carbamazepine, isoniazid, rifampin, phenytoin, phenobarbital (increased metabolism); H2-antagonists, omeprazole, antacids, didanosine (decreased absorption); inhibits CYP450 3A4 isoenzyme, thus increases effect of cyclosporine, tacrolimus (interferes with clearance); digoxin, warfarin and hypoglycemic agents (decreased metabolism); increased toxicity of terfenadine (recalled from US market), astemizole (recalled from US market), and cisapride (cardiotoxicity) Documented hypersensitivity; coadministration with cisapride may cause adverse cardiovascular effects (possibly death) PregnancyC - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus PrecautionsRare cases of serious cardiovascular adverse event, including death, ventricular tachycardia, and torsade de pointes have been observed because of increased terfenadine, astemizole, and cisapride concentrations induced by itraconazole; itraconazole solution and capsules should not be used interchangeably; PO solution is administered on an empty stomach and caps are taken with food Ketoconazole (Nizoral)An effective alternative agent in the treatment of immunocompetent patients with mild-to-moderate blastomycosis. In prospective randomized clinical trials conducted by the Mycoses Study Group, cure rates of 70-85% have been documented in patients treated with 400-800 mg/d. Relapse rates of 10-14% have been reported, and close follow-up monitoring is warranted for 1-2 years after therapy with ketoconazole. Adult400-800 mg/d PO; divide 800 mg/d in 2 doses PediatricNot established Drugs that decrease absorption (raise gastric pH), such as antacids, H2-receptor blockers; drugs that decrease serum concentrations of ketoconazole (rifampin, isoniazid); potent inhibitor of CYP450 3A4, drug concentrations that are increased by ketoconazole (phenytoin, cyclosporine, cisapride, astemizole (recalled from US market), digoxin, theophylline, terfenadine (recalled from US market), warfarin); drugs that cause hepatotoxicity; alcohol may cause disulfiramlike reactions Documented hypersensitivity; concomitant administration with terfenadine, astemizole, or cisapride PregnancyC - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus PrecautionsAdministration has been associated with hepatotoxicity, including some fatalities; high doses may depress adrenocortical function; risk of serious cardiac arrhythmias in patients receiving concomitant terfenadine, astemizole, or cisapride Fluconazole (Diflucan)The role of fluconazole therapy in blastomycosis is limited. In a small pilot study involving 23 patients, a successful outcome was noted in only 15 (65%) of cases. Better results were reported recently using higher dosages of fluconazole (400-800 mg/d). A successful outcome was noted for 34 (87%) of 39 patients treated for a mean duration of 8.9 mo. Although fluconazole demonstrates excellent CNS penetration, its role in the treatment of blastomycotic meningitis and cerebral abscesses is anecdotal. Adult400-800 mg/d PO PediatricNot established .
|