| Birt–Hogg–Dube syndrome=متلازمة بيرت هوك دووب |
|
|
Birt–Hogg–Dube syndrome
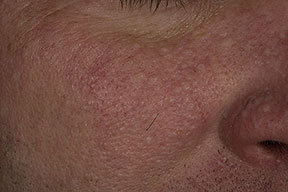
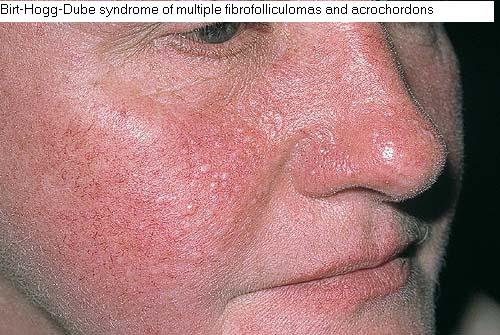
In 1977, Birt, Hogg, and Dubé reported small papular skin lesions distributed over the scalp, forehead, face, and neck in 15 of 70 members in a kindred study. Histologic examination of the lesions revealed fibrofolliculomas, trichodiscomas, and acrochordons. The presence of this triad has been termed Birt-Hogg-Dubé syndrome (BHDS). However, evidence suggests that these 3 lesions may actually represent only 1 lesion, the fibrofolliculoma, cut in various planes of section.3,8 Multiple or bilateral renal carcinomas, particularly chromophobe renal carcinoma and renal oncocytomas, have been reported in association with this syndrome. Pulmonary cysts and spontaneous pneumothoraces have also been increasingly reported manifestations of Birt-Hogg-Dubé syndrome.13,14,15,16 In one study, Toro et al reported 89% of patients with Birt-Hogg-Dubé syndrome had pulmonary cysts on CT scans. Further, the study demonstrated 24% of Birt-Hogg-Dubé syndrome patients and 34% of Birt-Hogg-Dubé syndrome family members screened for lung cysts had a history of spontaneous pneumothorax. PathophysiologySeveral authors have theorized that an ectodermal-mesodermal interaction stimulates hair development and growth of adjacent dermal structures. The cause of mesodermal proliferation is unknown, but autosomal dominant inheritance has been identified in patients with Birt-Hogg-Dubé syndrome (BHDS). Schmidt et al demonstrated that Birt-Hogg-Dubé syndrome maps to band 17p11.2.14,21 Further, Nickerson et al used recombination mapping to delineate the susceptibility focus to 700 kB on band 17p11.2. They also demonstrated a Birt-Hogg-Dubé syndrome tumor-suppressor protein, folliculin.22 Expression of the Birt-Hogg-Dubé syndrome protein has been widespread in a variety of tissues, including the kidneys, lungs, and skin. Baba et al identified the interaction of folliculin with the FLCN-interacting protein (FNIP1). FNIP1 interacts with 5'-AMP (activated protein kinase), which interacts with mammalian target of rapamycin (mTOR) and may be involved in cellular energy and nutrient sensing.24 In a mouse model, Baba et al have demonstrated homozygous loss of Birt-Hogg-Dubé syndrome protein results in uncontrolled cell proliferation and therefore may initiate tumorigenesis. While the poly C tract in exon 11 of the folliculin gene is the mutational hotspot, multiple other germline mutations have been detected
HistoryAsymptomatic, small, papular skin lesions develop gradually over the scalp, face, neck, and upper trunk. PhysicalMultiple, small (2-4 mm), white–to–flesh-colored, smooth, dome-shaped papules are distributed predominately over the scalp, face, oral cavity, neck, and upper trunk. Acrochordons are small, soft, furrowed, 1- to 2-mm papules that may occur on the eyelids, neck, axilla, and upper half of the trunk. Oral mucosal polyps, collagenomas, angiolipomas, and deforming lipomas also have been reported in association with Birt-Hogg-Dubé syndrome.30 CausesThe cause is unknown, but Birt-Hogg-Dubé syndrome (BHDS) is inherited in an autosomal dominant pattern. Several reports suggest Birt-Hogg-Dubé syndrome may result from the inactivation of a tumor-suppressor gene, which results in the cutaneous hamartomas associated with internal neoplasia. The Birt-Hogg-Dubé syndrome gene locus has been localized to band 17p11.2.
Imaging Studies
Other Tests
Procedures
Histologic FindingsFibrofolliculoma consists of a well-formed hair follicle with a dilated infundibulum containing laminated keratin. Radiating from the epithelium of the hair follicle are anastomosing epithelial strands of 2- to 4-mm thickness within a well-circumscribed mantle of loose mucinous connective tissue. These strands may arise from sebaceous epithelium deeply situated in the epidermis.33 The entire tumor is embedded in a fibrous or fibromucinous orb. In its classic description, trichodiscoma represents a small hamartomatous tumor of the hair disk (Haarscheibe). Pinkus et al described a constant topographic relationship of the hair follicle to the periphery of the papule. Other prominent features of trichodiscomas include a proliferation only of the fibrovascular component of the hair disk, small melanin-granule–containing cells in the substance of the tumor, and occasional myelinated nerves at the base of the lesion. Studies suggest that trichodiscomas also may be closely related to fibrofolliculomas, and their histologic appearance may relate to the plane of sectioning.34,35 Perifollicular fibroma classically is characterized by an unaltered hair follicle, commonly containing a hair shaft and surrounded by a distinct, circumferentially arranged, collagen fibrous sheath. Histologic study of perifollicular fibromas has revealed that sectioning techniques may skew interpretation of the lesions. Lesions described as perifollicular fibroma on horizontal sections were reexamined in vertical cuts and demonstrated histologic features similar to fibrofolliculoma, such as mantlelike strands of epithelium and sebaceous lobules at deeper levels of the epidermis. Thus, the entity of perifollicular fibroma may represent a transverse cut of a fibrofolliculoma, rather than a perifollicular fibroma. |