|
Benign mucosal pemphigoid= الفقاعاني المخاطي الحميد |
 |
 |
 |
              
Cicatricial pemphigoid
Cicatricial pemphigoid (CP) refers to a group of rare chronic autoimmune blistering diseases that predominately affects the mucous membranes, including the conjunctiva, and occasionally the skin. Patients with cutaneous involvement present with tense blisters and erosions, often on the head and the neck or at sites of trauma. Scarring of the mucous membranes is common, hence the designation cicatricial, which can lead to decreased vision, blindness, and supraglottic stenosis with hoarseness or airway obstruction. The first international consensus on mucous membrane pemphigoid was published in 2002.1
See the illustration below depicting ocular cicatricial pemphigold disease
The classification of cicatricial pemphigoid patients has been difficult because some patients with other autoimmune blistering diseases, including bullous pemphigoid (BP) and epidermolysis bullosa acquisita (EBA), may have mucosal involvement. Also, clinical heterogeneity exists in the clinical manifestations of this disease, with some patients presenting with ocular involvement and others with oropharyngeal involvement. The heterogeneity in clinical manifestations does not appear to be linked to the heterogeneity of the target antigens alone.
Pathophysiology
As in other autoimmune diseases, environmental factors combined with genetic susceptibility lead to development of autoantibodies. By direct immunofluorescence (DIF) study, antibodies bound in a linear band at the epidermal-dermal junction have been found in patients with cicatricial pemphigoid, as depicted below. By immunoelectron microscopy, these antibodies are found in the lamina lucida. In some patients, autoantibodies extend to the lamina densa. When detectable, circulating autoantibodies are present in a low titer.
Different epithelial membrane zone components have been recognized by antibodies in patients with cicatricial pemphigoid, including bullous pemphigoid antigen 1 and 2 (BPAG1 and BPAG2), laminin 5, laminin 6, type VII collagen, b4 integrin subunit, and antigens with unknown identities (a 45-kd protein, uncein, a 168-kd epithelial protein, and a 120-kd epithelial protein). While circulating autoantibodies in a given patient tend to target a single antigen, sera of patients with same clinical features may target different autoantigens
History
- Patients with cicatricial pemphigoid typically present with persistent, painful erosions on the mucous membranes. The clinical manifestations are dependent on the sites involved.
- Patients with ocular involvement may present with pain or the sensation of grittiness in the eye and conjunctivitis. Erosions may be seen on the conjunctival surface. Early changes include keratinization of the conjunctiva and shortening of the fornices. Later, patients develop entropion with subsequent trichiasis.
- Patients often present after ocular surgery, especially for cataracts, with severe inflammation of the eye or eyes and scar formation. With progressive scarring, patients develop symblepharon (fibrous tracts that tether bulbar and conjunctival epithelium), synechiae (adhesion of the iris to the cornea or the lens), and ankyloblepharon (a fixed globe). See images below.
- Lacrimal gland and duct involvement leads to decreased tear and mucous production. Diminished tear formation leads to ocular dryness and further trauma.
- The end result of ocular involvement is opacification and blindness. Some patients with ocular disease may represent a subset of patients with cicatricial pemphigoid who do not develop oropharyngeal, other mucous membrane, or cutaneous disease.
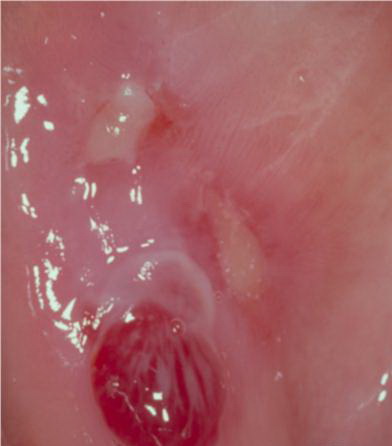
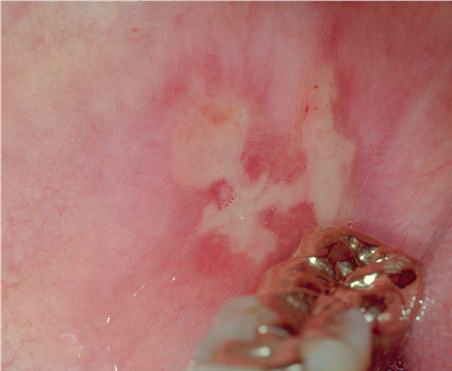
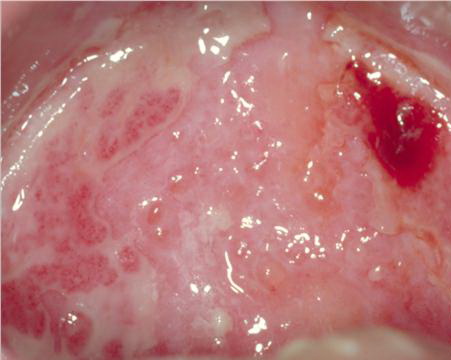
- Mouth involvement presents as recurrent, painful erosions. The gingivae are most commonly involved, followed by the palate and the buccal mucosa; however, any mucosal site in the mouth may blister. Involvement of the oropharynx may present with hoarseness or dysphagia. Progressive scarring disease may lead to esophageal stenosis requiring dilatation procedures. Supraglottic involvement may lead to airway compromise requiring tracheostomy.
- Nasal involvement may manifest as epistaxis, bleeding after blowing the nose, nasal crusting, and discomfort. Other mucosal sites, such as the perianal area or the genitalia, may be involved.
- Skin lesions develop in approximately one third of patients with cicatricial pemphigoid, manifesting as tense vesicles or bullae that may be hemorrhagic. Blisters may heal with scarring or milia. Scalp involvement may lead to alopecia. Pruritus at the sites of blisters or generalized pruritus may be present.
- Cutaneous cicatricial pemphigoid involving the head and the neck without mucosal involvement is known as the Brunsting-Perry variant of localized BP. Patients are predominately elderly and male. Patients present with a chronic, recurrent vesiculobullous eruption on the head and the neck that heals with atrophic scarring. Patients with this disorder have histologic immunofluorescent and immunoelectron microscopic features similar to other patients with cicatricial pemphigoid.
- Early ocular lesions may manifest as conjunctivitis, progressing to keratinization of the corneal epithelium and shortening of the corneal sulcus (see first image below). Progressive ocular disease leads to entropion (see first image below) and progressive corneal injury secondary to trichiasis. With persistent disease activity, synchesis and symblepharon occur (see second image below). Long term, ankyloblepharon (a fixed globe) may occur (see third image below). Patients with pure ocular involvement may constitute a distinct subset of patients with cicatricial pemphigoid. These patients are distinct from patients with classic BP because they have a lower frequency of immunoglobulin G (IgG) and C3 as depicted by DIF, and they are usually negative for circulating autoantibodies as depicted by indirect immunofluorescence (IDIF). These patients do not have detectable reactivity to BP antigens.
- Cicatricial pemphigoid is an autoimmune blistering disease associated with autoantibodies directed against basement membrane zone target antigens. Autoantibodies of the IgG subclass, particularly IgG4, are associated with cicatricial pemphigoid; however, IgA antibodies have also been detected. The 2 major antigens associated with cicatricial pemphigoid are BPAG2 and epiligrin (laminin-5). Patients with clinical features of cicatricial pemphigoid may have antibodies directed against BPAG1 or the EBA antigen (type VII collagen). No clinical difference between patients with anti-BPAG2 and antiepiligrin reactivity is present.
- BPAG2 is also known as collagen XVII. It is a 180-kd hemidesmosomal protein with multiple extracellular collagenous domains.2 BPAG2 is also a major target antigen for patients with BP and linear IgA bullous dermatosis. Patients with cicatricial pemphigoid react with epitopes on BPAG2 distinct from those associated with BP and linear IgA bullous dermatosis. Recent studies suggest that BPAG2 is cleaved to form a 120-kd fragment that contains the cicatricial pemphigoid epitope. Circulating autoantibodies in patients with autoantibodies specific for BPAG2 bind to the epidermal side of salt-split skin as depicted by IDIF study.
- A subset of patients with cicatricial pemphigoid reacts with laminin-5. These patients have circulating autoantibodies that bind to the dermal side of salt-split skin as depicted by IDIF study. By immunoelectron microscopy, these autoantibodies deposit at the lower lamina lucida, extending to the lamina densa. Laminin-5 contains disulfide-linked alpha, beta, and gamma chains, of which the alpha subunit is the major site of cicatricial pemphigoid reactivity. Laminin-5 plays a major role in the adhesion of human keratinocytes to the dermis by binding alpha-6-beta-4 integrin. Because defects in laminin-5 are associated with junctional epidermolysis bullous, one group has suggested calling cicatricial pemphigoid associated with antiepiligrin autoantibodies acquired junctional EB; however, most clinicians refer to this disease as antiepiligrin cicatricial pemphigoid.
- Autoantibodies specific for epiligrin and BPAG2 are believed to be important in blister formation. Lazarova et al3 have developed an animal model of antilaminin-5 cicatricial pemphigoid in which passive transfer of rabbit antilaminin-5 into neonatal mice leads to a subepidermal blistering disease with features consistent with cicatricial pemphigoid. Passive transfer of antilaminin-5 antibodies to mast cell and complement deficient neonatal mice can also induce blistering, suggesting a direct effect of the circulating autoantibodies in inducing dermal-epidermal cleavage.
- The incidence of the HLA haplotype HLA-DQB1*0301 is increased in patients with ocular cicatricial pemphigoid. This HLA haplotype may be important in the presentation of specific epitopes on target antigens in the generation of an autoimmune response; however, the precise events relevant in the initiation of autoantibody production in patients with this disease are unknown.
Physical
- Nasal involvement can be detected as erosions and crusting in the nasal vestibule, best seen by nasal speculum examination.
- Oral erosions often begin on the gingiva, particularly near the teeth. Erosions can also be seen on the palate, the buccal mucosa, the lips, the posterior part of the pharynx, the tongue, and the floor of the mouth. Intact blisters are rarely seen, but they may appear flaccid or tense.
- On the genitalia, painful erosions involving the clitoris, the labia, the glans, or the shaft of the penis may be seen. Perianal involvement manifests as perianal blisters and erosions.
- On the skin, tense blisters or erosions may be seen on either normal-appearing skin or erythematous plaques. Common sites include the scalp, the head, the neck, the distal extremities, or the trunk. In patients with active disease, erosions may be persistent and difficult to heal. Scarring and milia frequently develop in this condition and are helpful in clinically differentiating cicatricial pemphigoid from BP and linear immunoglobulin A (IgA) bullous dermatosis, both of which do not tend to scar.
- Localized cicatricial pemphigoid on the head and the neck is known as Brunsting-Perry cicatricial pemphigoid. This disease heals with scarring and milia.
Causes
Laboratory Studies
- The histologic findings, DIF results, and IDIF results of cicatricial pemphigoid, BP, and EBA are similar; differentiation between these 3 entities depends on the clinical presentation.
- Criteria for the diagnosis of cicatricial pemphigoid include an appropriate clinical presentation, histology demonstrating a subepidermal blistering process (as described below), and DIF results showing continuous deposits of any one or the combination of the following along the epithelial basement membrane zone: IgG, IgA, and/or C3. DIF study can be used to categorize the process as an autoimmune blistering disease, but it cannot be used to discriminate between cicatricial pemphigoid, BP, or EBA.
- IDIF study of patients' sera depicts circulating antibasement membrane zone specific for IgG in 20% of patients, and, when present, it usually has a low titer (1:10-1:20).
Imaging Studies
- For evaluation of the upper airway or the esophagus, CT scans, barium swallows, or other imaging studies may be helpful. In patients with antiepiligrin cicatricial pemphigoid, imaging may be required as part of malignancy search.
Other Tests
- DIF study should be performed on noninvolved perilesional skin or mucous membrane. Patients with cicatricial pemphigoid typically demonstrate linear deposits of complement and IgG at the dermal-epidermal junction. The most commonly assayed complement component is C3; however, C4, properdin, and other complement components have been described. Linear deposits of IgG are detectable in 25% of patients. Linear deposits of IgA, in addition to IgG, have been reported in 20% of patients in one series. This pattern of DIF is also seen in patients with BP and EBA, and DIF assay cannot be used to differentiate among these disorders. Conjunctival specimens have been reported to be less sensitive than biopsy specimens of oral mucosa on DIF results.
- IDIF assay detects the presence of circulating antibodies directed against normal epithelial basement membrane in the sera of patients who are affected. In patients with cicatricial pemphigoid, IDIF assay reveals circulating IgG in 20% of patients, typically a low titer. When healthy human skin preincubated in 1 mol/L sodium chloride (salt-split skin) is used as a substrate, autoantibodies in patients with cicatricial pemphigoid associated with reactivity to BPAG2 bind to the epidermal roof. IDIF results demonstrate a similar localization in patients with BP. Patients with autoantibodies associated with epiligrin have circulating autoantibodies that bind to the blister floor, similar to that in patients with EBA. One laboratory has reported an increased sensitivity by IDIF study by concentrating serum samples prior to assay.
- Immunoblot (Western blot), immunoprecipitation, and immunoelectron microscopy are investigational tools used to better define target antigens. By immunoblot (Western blot) and immunoprecipitation, patients with cicatricial pemphigoid can have autoantibodies directed against BPAG2 (180 kd), BPAG1 (230 kd), and epiligrin (a chain of laminin-5). Enzyme-linked immunoassays using recombinant target antigens may ultimately be available to characterize autoantibody reactivity.
- Routine laboratory studies are not helpful in establishing the diagnosis of cicatricial pemphigoid. Most hematologic studies are within the reference range. Laboratory values that may be elevated include immunoglobulins, erythrocyte sedimentation rate, and acute phase reactants.
Histologic Findings
Biopsy of the edge of an early blister typically reveals a noninflammatory, subepidermal blister. When present, the inflammatory infiltrate localizes to the dermal-epidermal junction and the perivascular areas. This histologic feature can also be seen in other autoimmune subepidermal blistering diseases, including cell-poor BP, EBA, and linear IgA bullous dermatosis. The histologic features of porphyria cutanea tarda and variegate porphyria may also resemble cicatricial pemphigoid.
Medical Care
The goal of treatment is to suppress extensive blister formation, to promote healing, and to prevent scarring. The lowest dose of medication to suppress disease activity and to minimize the risk for the patient should be used. This disorder is extremely difficult to treat. Even with optimum control, blisters may continue to develop in some patients. The risks and the benefits of therapy must always be evaluated for each patient.
Wound care of erosions includes daily gentle cleaning or compresses, topical agents to promote wound healing, and biologic dressings. The goals of wound care are to minimize trauma to the surrounding skin, to promote healing, and to diminish scarring.
Increased risk of malignancies has been documented in patients with antiepiligrin cicatricial pemphigoid, especially in the first year of disease; hence, appropriate screening is warranted.
Surgical Care
Surgical intervention may be required to improve functioning or to prevent further morbidity. Such intervention is directed at the sequelae of chronic blistering.
- Patients with cicatricial pemphigoid and ocular involvement require ongoing ophthalmologic care. Surgical intervention to ablate ingrown eyelashes prevents further ocular damage. Procedures to release entropion have been successful. Tsubota et al4 recently reported the long-term outcome in patients with cicatricial ocular disorders treated with limbal allografts. The transfer of epithelial stem cells restored useful vision in these patients, including several patients with ocular cicatricial pemphigoid. Care should be taken to control the inflammatory component of the disease before and immediately after surgery because patients with cicatricial pemphigoid frequently experience flare-ups after surgery.
- Patients with upper airway disease may develop respiratory compromise requiring tracheostomy.
- Patients with esophageal obstruction may require dilatation procedures.
Consultations
The management of cicatricial pemphigoid requires a coordinated team approach. Specific consultations are dictated by the phenotype of the disease and the target organ or organs that are involved.
- The patient management team typically includes a dermatologist with expertise in this area; an internist to assist with monitoring therapy, adverse effects of medications, and the patient's overall health; an ophthalmologist for ocular disease; an otolaryngologist for upper airway evaluation and management; and a dentist for oral disease.
- Additional specialists, such as a gynecologist (vulvar disease), a gastroenterologist (esophageal involvement), and an endocrinologist (prophylaxis of osteoporosis in patients receiving chronic systemic corticosteroids), may be indicated.
Diet
- Although no dietary restrictions are necessary, patients with oral disease may benefit from avoiding foods high in acid, such as tomatoes and orange juice, and foods with hard surfaces that may mechanically traumatize the oral epithelium, such as chips, nuts, raw vegetables, and uncut fruit.
- Patients on oral prednisone should maintain adequate calcium and vitamin D intake through diet and supplements. The daily calcium requirement in patients with no history of kidney stones is 1.5 g/d, and the daily minimum dose of vitamin D is 800 IU/d.
Activity
Patients are encouraged to lead as normal a life as possible; however, cutaneous and mucosal blisters may be induced by trauma. Contact lenses, dental plates, or bridges may precipitate or exacerbate mucosal disease. Patients may benefit by minimizing activities, such as contact sports, that traumatize the skin and precipitate blistering. Nontraumatic exercises, such as swimming or aquatic exercises, may be beneficial.
Medication
Patients with mild localized disease may benefit from topical steroids (eg, triamcinolone [Kenalog in Orabase]) in gel-based topical agents for oral disease or in ointment-based topical steroids for cutaneous disease. Intralesional steroids can be administered as triamcinolone acetonide (Kenalog susp) 10 mg/mL injected weekly or biweekly for oral and cutaneous lesions. Patients with more extensive disease and progressive scarring require systemic therapy with prednisone and/or steroid-sparing agents, such as cyclophosphamide, azathioprine, cyclosporin, mycophenolate mofetil. Evidence from 2 small randomized controlled trials indicates that ocular cicatricial pemphigoid responds best to cyclophosphamide, while mild-to-moderate disease seems effectively suppressed by treatment with dapsone.
High-dose intravenous immune globulin has been used successfully in the treatment of cicatricial pemphigoid in patients who were refractory to other therapies. Immunosuppressive agents should be prescribed and monitored by physicians familiar with these medications. The 2002 consensus statement on cicatricial pemphigoid1 reports expert panel opinion on the management of the disease.
Anti-inflammatory Agents
These agents decrease the inflammatory response.
Triamcinolone topical (Kenalog, Kenalog in Orabase)
Agent for mild disease or used as an adjuvant in patients receiving concurrent systemic therapy. Decreases inflammation by suppressing migration of polymorphonuclear leukocytes and reversing capillary permeability.
Adult
Apply topically to gingiva and oral blisters tid
Pediatric
Apply as in adults
Documented hypersensitivity; fungal, viral, and bacterial skin infections; not indicated in extensive mucosal involvement
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Do not use in decreased skin circulation; prolonged use, applying over large areas, and using potent steroids and occlusive dressings may result in systemic absorption; systemic absorption may cause Cushing syndrome, reversible HPA-axis suppression, hyperglycemia, and glycosuria
Dapsone (Avlosulfon)
DOC for ocular cicatricial pemphigoid and often beneficial in patients with oral mucosal disease. Bactericidal and bacteriostatic against mycobacteria. Mechanism of action is similar to that of sulfonamides where competitive antagonists of PABA prevent formation of folic acid, inhibiting bacterial growth.
Adult
50 mg PO qd initial; increase to 100 mg/d as tolerated
Pediatric
>1 month: 1 mg/kg/d PO; not to exceed 100 mg
May inhibit anti-inflammatory effects of clofazimine; hematologic reactions may increase with folic acid antagonists, eg, pyrimethamine (monitor for agranulocytosis during second and third months of therapy); probenecid increases toxicity; trimethoprim with dapsone may increase toxicity of both drugs; because of increased renal clearance, levels may significantly decrease when administered concurrently with rifampin; concomitant administration of zidovudine may increase risk of hematologic toxicity; amprenavir and saquinavir may inhibit cytochrome P4503A (CYP3A), the hepatic isoenzyme group with major activity related to dapsone metabolism, thereby leading to increased dapsone serum concentrations and potential toxicity
Documented hypersensitivity; known G-6-PD deficiency (assay for G-6-PD activity prior to initiation of therapy)
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Associated with a variety of systemic toxicities, including agranulocytosis, anemia, methemoglobinemia, hepatitis, and neuropathy; patients may experience headache and/or GI distress on initiation of therapy; perform weekly blood counts (first mo), then monthly WBC counts (6 mo), then semiannual WBC counts; discontinue if a significant reduction in platelets, leukocytes, or hematopoiesis occurs; caution in methemoglobin reductase deficiency, G-6-PD deficiency, or hemoglobin M because of high risk for hemolysis and Heinz body formation; caution in patients exposed to other agents or conditions (eg, infection, diabetic ketosis) capable of producing hemolysis; peripheral neuropathy can occur (rare); phototoxicity may occur when exposed to UV light; pancreatitis may occur; various forms of renal complications including acute renal failure, acute tubular necrosis, and oliguria have occurred with dapsone use
Prednisone (Deltasone, Orasone, Sterapred)
May decrease inflammation by reversing increased capillary permeability and suppressing PMN activity.
Adult
20-40 mg/kg/d PO qam or in divided doses initially; if no response, dose is typically increased by 50% q3-5d
Pediatric
1-2 mg/kg PO qd or divided bid/qid; taper over 2 wk as symptoms resolve
Coadministration with estrogens may decrease clearance; when used with digoxin, digitalis toxicity secondary to hypokalemia may increase; phenobarbital, phenytoin, and rifampin may increase the metabolism of glucocorticoids (consider increasing maintenance dose); monitor for hypokalemia with coadministration of diuretics; coadministration with ritonavir may significantly increase serum concentrations of prednisone; concomitant therapy with montelukast may result in severe peripheral edema; clarithromycin may increase risk of psychotic symptoms
Postmarketing surveillance reports indicate that risk of tendon rupture may be increased in patients receiving concomitant fluoroquinolones and corticosteroids, especially elderly patients; administration of asparaginase concurrently with or before prednisone therapy may result in increased toxicity
Documented hypersensitivity; viral, fungal, tubercular skin, or connective tissue infections; peptic ulcer disease; hepatic dysfunction
Pregnancy
B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions
May unmask hypertension or diabetes or exacerbate peptic ulcer disease and tuberculosis; long-term sequelae associated with long-term steroid use include osteoporosis, cataracts, and pituitary-hypothalamic axis suppression; with high doses, patients may develop a steroid psychosis and are at increased risk of infections, particularly when oral steroids are used in conjunction with other immunosuppressants; frequently monitor patient's blood sugar level, blood pressure, and weight; monitor for Cushing syndrome
Immunosuppressants
These agents inhibit immune reactions resulting from diverse stimuli.
Azathioprine (Imuran)
Antagonizes purine metabolism and inhibits synthesis of DNA, RNA, and proteins. May decrease proliferation of immune cells, which results in lower autoimmune activity.
Adult
1 mg/kg/d PO for 6-8 wk; increase by 0.5 mg/kg q4wk until response or dose reaches 2.5 mg/kg/d
Alternatively, may dose on RBC thiopurine methyltransferase activity level checked prior to initiating treatment
Pediatric
Administer as in adults
Toxicity increases with allopurinol; concurrent use with ACE inhibitors may induce severe leukopenia; may increase levels of methotrexate metabolites and decrease effects of anticoagulants, neuromuscular blockers, and cyclosporine; coadministration with mycophenolate may increase toxicity; alfalfa, black Cohosh, and echinacea may reduce immunosuppressive drug effectiveness
Documented hypersensitivity; deficiency of thiopurine methyltransferase (can result in severe myelosuppression and leukopenia); history of treatment with alkylating agents
Pregnancy
D - Fetal risk shown in humans; use only if benefits outweigh risk to fetus
Precautions
Increases risk of neoplasia; caution with liver disease and renal impairment; hematologic toxicities may occur; hepatotoxicity and pancreatitis reported
Cyclosporine (Sandimmune, Neoral)
Demonstrated to be helpful in a variety of skin disorders. Cyclic polypeptide that suppresses some humoral immunity and, to a greater extent, cell-mediated immune reactions, such as delayed hypersensitivity, allograft rejection, experimental allergic encephalomyelitis, and graft-vs-host disease for a variety of organs. For children and adults, base dosing on ideal body weight.
Adult
3-9 mg/kg/d PO
Pediatric
Administer as in adults
Carbamazepine, phenytoin, isoniazid, rifampin, and phenobarbital may decrease concentrations; azithromycin, itraconazole, nicardipine, ketoconazole, fluconazole, erythromycin, verapamil, grapefruit juice, diltiazem, aminoglycosides, acyclovir, amphotericin B, and clarithromycin may increase toxicity; acute renal failure, rhabdomyolysis, myositis, and myalgias increase when taken concurrently with lovastatin
Documented hypersensitivity; uncontrolled hypertension or malignancies; do not administer concomitantly with PUVA or UV-B radiation in patients with psoriasis because it may increase risk of cancer
Pregnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Evaluate renal and liver functions often by measuring BUN, serum creatinine, serum bilirubin, and liver enzyme levels and blood pressure; may increase risk of infection and lymphoma; reserve IV use only for those who cannot take PO; adverse effects include nephrotoxicity, hypertension, hepatotoxicity, gingival enlargement, hyperkalemia, hypomagnesemia, pancreatitis, and paresthesia; factors that may increase risk for neurotoxicity from cyclosporine include hypomagnesemia, hypocholesterolemia, fever, infection, hypertension, intravenous administration, and rapidly increasing cyclosporine blood levels; caution with medications metabolized by cytochrome P450 3A4
Cyclophosphamide (Cytoxan, Neosar)
Chemically related to nitrogen mustards. As an alkylating agent, the mechanism of action of the active metabolites may involve cross-linking of DNA, which may interfere with growth of normal and neoplastic cells.
Adult
1-5 mg/kg/d IV; alternatively 2.5-3 mg/kg/d PO divided qid
Pediatric
Administer as in adults
Allopurinol may increase risk of bleeding or infection and enhance myelosuppressive effects; may potentiate doxorubicin-induced cardiotoxicity; may reduce digoxin serum levels and antimicrobial effects of quinolones; chloramphenicol may increase half-life while decreasing metabolite concentrations; may increase effect of anticoagulants; coadministration with high doses of phenobarbital may increase rate of metabolism and leukopenic activity; thiazide diuretics may prolong cyclophosphamide-induced leukopenia and neuromuscular blockade by inhibiting cholinesterase activity; concurrent use of NSAIDs has resulted in increases in cyclosporine levels, nephrotoxicity, and increased plasma creatinine concentrations
Concomitant use of ACE inhibitors may decrease renal function; coadministration with nevirapine and St. John's wort may reduce immunosuppressive drug effectiveness
Increased risk of infection by live vaccine; coadministration with trastuzumab may increase cardiac toxicity; coadministration with tamoxifen may increase risk of thromboembolism
Documented hypersensitivity; severely depressed bone marrow function
Pregnancy
D - Fetal risk shown in humans; use only if benefits outweigh risk to fetus
Precautions
Regularly examine hematologic profile (particularly neutrophils and platelets) to monitor for hematopoietic suppression; regularly examine urine for RBCs, which may precede hemorrhagic cystitis; adverse effects include oligospermia or azoospermia, cardiomyopathy, infectious disease, interstitial pneumonia, increase risk of malignancy, possibility of increased toxicity in adrenalectomized patients
Mycophenolate (CellCept)
Inhibits purine synthesis and proliferation of human lymphocytes.
Adult
1-1.5 g PO bid
Pediatric
<3 months: Not established
>3 months : 600 mg/m2/dose susp PO bid; not to exceed 2 g/d PO
Alternatively, administer according to BSA
>3 months or 1.25-1.5 m2: 750 mg PO cap bid
>3 months or >1.5 m2: 1000 mg PO cap or tab bid
.
|
|
|
|