
















































































Tinea Pedis and Tinea
Manus
Tinea pedis is a dermatophytosis of the feet, whereas tinea manus affects the palmar and interdigital areas of the hand.
EPIDEMIOLOGY
Present worldwide, tinea pedis and tinea manus are the most common dermatophytoses. The prevalence of tinea pedis is approximately 10 percent, primarily attributable to modern occlusive footwear, although increased worldwide travel has also been implicated. The incidence of tinea pedis is higher among those using communal baths, showers, or pools.
Tinea manus may be acquired by direct contact with an infected person or animal, the soil, or autoinoculation. However, it is nearly always associated with tinea pedis and occurs most commonly in the hand used to excoriate the feet.
ETIOLOGY
Tinea pedis and tinea manus are caused predominantly by T. rubrum (most common), T. mentagrophytes, and E. floccosum.
CLINICAL FINDINGS
Tinea pedis may present as any of four forms, or a combination thereof.
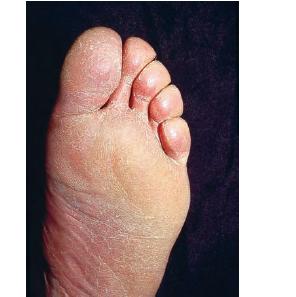
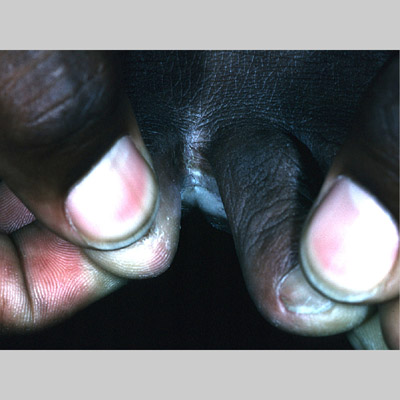
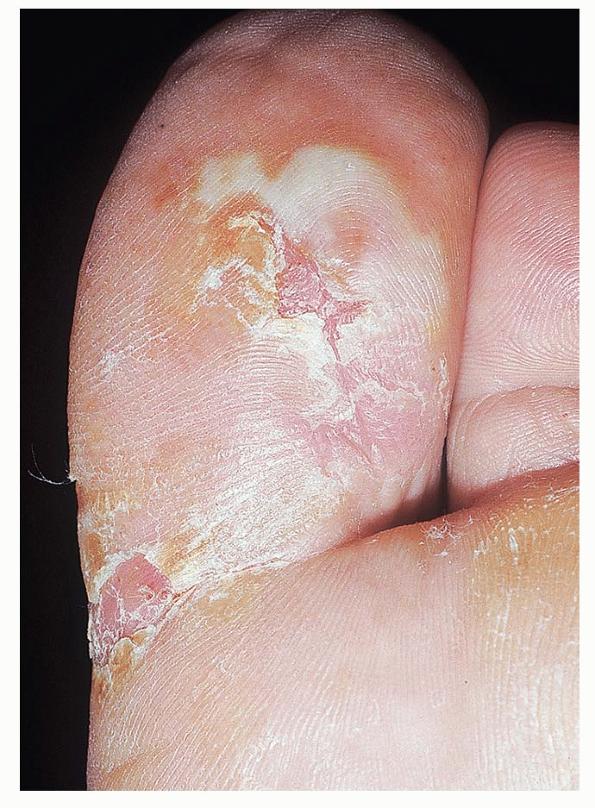
Chronic Intertriginous Type (Interdigital Type).
The most common presentation of tinea pedis, the chronic intertriginous
type, begins as scaling, erosion, and erythema of the interdigital and subdigital skin of the feet, particularly between the lateral three toes. Under appropriate conditions, the infection will spread to the adjacent sole or instep, rarely involving the dorsum. Occlusion and bacterial co-infection soon produce the interdigital maceration, pruritus, and malodor of dermatophytosis complex
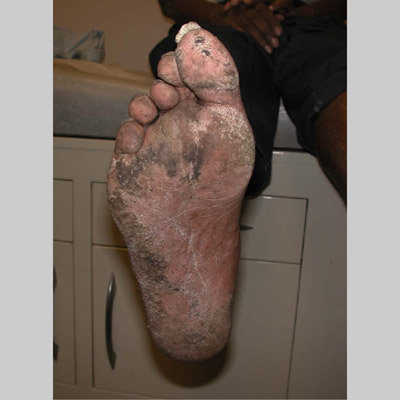
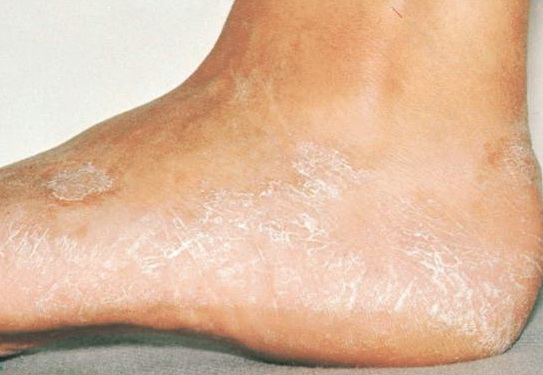
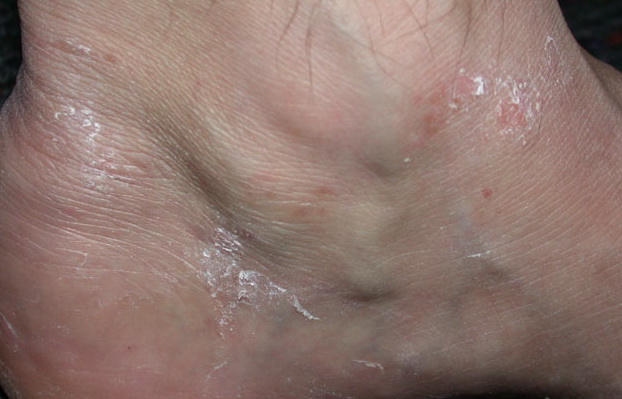
Chronic Hyperkeratotic Type.
Usually bilateral with patchy or diffuse scaling limited to the thick skin, soles, and the lateral and medial aspects of the feet, this is also known as “moccasin-type” tinea pedis. T. rubrum, the most common etiology, produces very few minute vesicles, leaving collarettes of scale less than 2 mm in diameter. Erythema is variable.
Unilateral tinea manuum commonly occurs in association with hyperkeratotic tinea pedis, resulting in the “two feet-one hand syndrome” . When tinea manus extend to the dorsum of a hand, it assumes the clinical pattern of tinea corporis . Oral antifungals are often required for treatment due to the high incidence of concomitant onychomycosis and relapse.
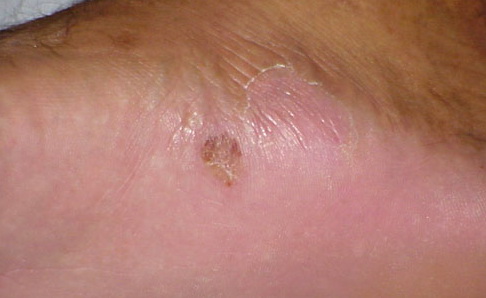
Vesiculo-Bullous Type.
The vesiculo-bullous type of tinea pedis, typically caused by T. mentagrophytes, features tense vesicles larger than 3 mm in diameter, vesiculopustules, or bullae on the thin skin of the sole and periplantar areas . It is rarely reported in childhood, but the most common etiologic agent in childhood is T. rubrum.
Acute Ulcerative Type.
Rampant bacterial co-infection, most often from Gram negatives in combination with T. mentagrophytes, produces vesiculopustules and large areas of purulent ulceration on the plantar surface. Cellulitis, lymphangiitis, lymphadenopathy, and fever are frequently associated.
The vesiculo-bullous and acute ulcerative types commonly produce a vesicular id reaction, either as a dyshidroticlike distribution on the hands or on the lateral foot or toes.
LABORATORY TESTS
For vesiculo-bullous lesions, examination of the roofs yields the highest rate of positivity on KOH examination.
PATHOLOGY
Histologically, hyperkeratotic tinea pedis or tinea manuum is characterized by acanthosis, hyperkeratosis, and a sparse, chronic, superficial perivascular infiltrate in the dermis. Vesiculo-bullous forms display spongiosis, parakeratosis, and sub-corneal or spongiotic intraepithelial vesiculation. With both types, foci of neutrophils are occasionally seen in the stratum corneum. PAS or methenamine silver staining demonstrates fungal organisms.
Differential Diagnosis of Tinea Manus et Pedis
Most Likely
· Interdigital: Psoriasis, soft corns, bacterial co-infection, candidiasis, erythrasma
· Hyperkeratotic: Psoriasis, hereditary or acquired keratodermas of the palms and soles, dyshydrosis
· Vesiculo-bullous: Pustular psoriasis, palmoplantar pustulosis, bacterial pyodermas
Consider
· Pityriasis rubra pilaris, contact dermatitis, peridigital dermatitis, atopic dermatitis
Rule Out
· Reiter syndrome