













MEASLES
Epidemiology
Measles, or rubeola, has a worldwide distribution and remains a leading public health burden, with 30 to 40 million cases and 530,000 deaths in 2003. The risk of mortality is highest in developing countries, with most deaths due to complications of the disease.
Before the development of a vaccine, measles epidemics occurred every 2 to 5 years during winter and spring months in children 5 to 9 years old.2,3 There continues to be a decline in the number of reported cases in the United States each year as vaccination strategies have improved, particularly in immigrant populations. During 2004, a total of 37 cases were reported to the Centers for Disease Control and Prevention by local and state health departments.4 Improved immunization programs in developing countries have also prevented outbreaks and reduced measles-associated morbidity and mortality.
Etiology and Pathogenesis
Measles virus, a member of the Paramyxoviridae family, is a heat-labile virus with an RNA core and outer lipoprotein envelope. Measles is spread by direct or airborne contact with infectious droplets. The incubation period is typically 8 to 12 days, with patients being contagious from 1 to 2 days before onset of symptoms to 4 days after appearance of the rash.3 Both humoral and cell-mediated immunity are needed to control measles virus infection. Immunoglobulin M (IgM) antibodies are detected initially with onset of the rash, followed by a rise in measles-specific IgG titers. The humoral response controls viral replication and confers antibody protection, whereas the cell-mediated response eliminates infected cells.2 A transient immunosuppression occurs during measles virus infection, causing depressed delayedtype hypersensitivity and T-cell counts as well as an increased risk of bacterial infections. This process, as well as long-term immunity against measles, is not well understood but may be due to a weak T helper 1 response to the virus.
Clinical Findings
HISTORY
The prodrome is typically characterized by fever [up to 40°C to 40.5°C (104°F to 105°F)], malaise, conjunctivitis (palpebral, extending to lid margin), coryza, and cough (brassy or barking), which may last up to 4 days.2,3 Koplik spots, the pathognomonic enanthem of measles, begin as small, bright red macules that have a 1- to 2-mm blue-white speck within them. They are typically seen on the buccal mucosa near the second molars 1 to 2 days before and lasting 2 days after the onset of the rash Individuals with pre-existing partial immunity (e.g., patients who received exogenous immunoglobulin) may have less severe symptoms but a prolonged incubation period (14 to 20 days). Conversely, immunosuppressed patients may have more severe disease and can present without the typical rash.
CUTANEOUS LESIONS
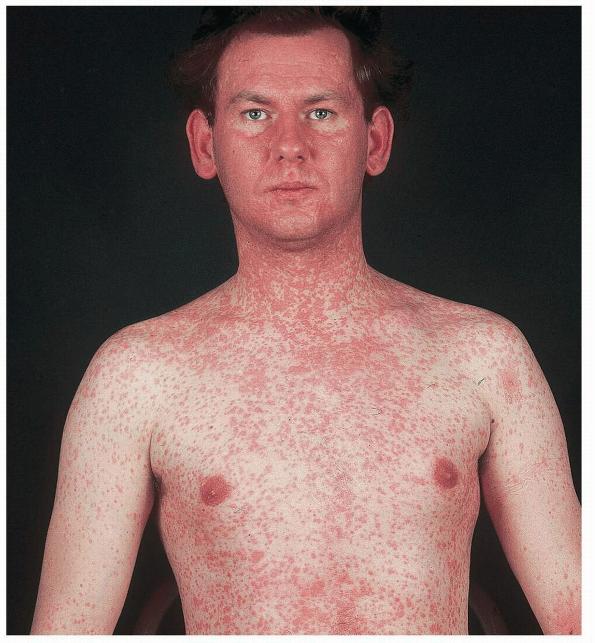
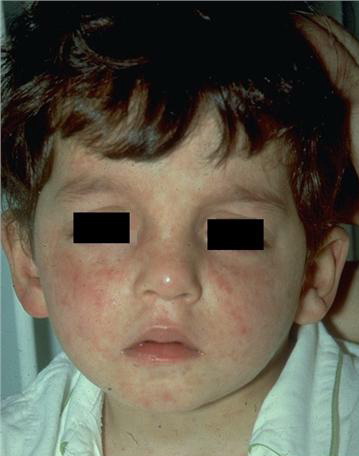
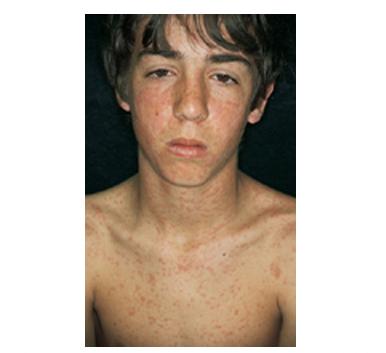
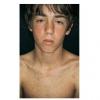
The exanthem is characterized by erythematous, non-pruritic, macules and papules that begin on the forehead and behind the ears .
The rash quickly progresses to involve the neck, trunk, and extremities . The hands and feet are involved. Lesions may coalesce, especially on the face and neck . The rash usually peaks within 3 days and begins to disappear in 4 to 5 days after the order of its appearance. Desquamation may occur as the rash resolves.
RELATED PHYSICAL FINDINGS
The entire illness may last up to 10 days, with some individuals also having vomiting, diarrhea, abdominal pain, splenomegaly, pharyngitis, and generalized lymphadenopathy. Immunosuppressed patients are at higher risk for pneumonitis, encephalitis, and other fatal complications. Viral shedding may also be more persistent in these individuals.
Atypical measles infection is rare, but seen in individuals who received formalin-inactivated measles vaccine (1963 to 1967) and were subsequently exposed to wild-type virus. Symptoms are often more severe with high fever, interstitial pneumonia, pleural effusions, extremity edema, hepatitis, and hyperesthesias occurring more commonly. Coryza, conjunctivitis, and Koplik spots are usually not present. The rash may be maculopapular, hemorrhagic, vesicular, or urticarial and spreads centripetally, making it difficult to distinguish from Rocky Mountain spotted fever.2
Laboratory Tests
Laboratory abnormalities may include monocytosis, leucopenia, and thrombocytopenia. During the prodrome stage, virus can be found in nasopharyngeal secretions, blood, and urine. The pharyngeal virus shedding ends by the second day of the rash. Virus may be seen in the urine until 4 days after rash onset. Viral culture has a low sensitivity for finding the virus. Indirect enzyme-linked immunoassay (ELISA), polymerase chain reaction (PCR), and real-time (RT)-PCR assays can detect measles virus in clinical specimens such as nasopharyngeal secretions, blood, and urine.8 Serologic studies demonstrate measles virus infection with a documented increase in IgM and/or IgG antibody titers. IgM increases with the onset of the rash and lasts approximately 1 month whereas IgG appears 2 weeks after rash onset and peaks 4 to 6 weeks later.3,9 Many laboratories may have access to viral immunofluorescence tests that quickly detect measles in throat or nasopharyngeal specimens.10 In the United States, measles should be reported to the local health department.
Complications
Age-specific rates of complications are highest among children less than 5 years old and adults over 20 years. The most common complications of measles virus infection are otitis media, pneumonia, laryngotracheobronchitis, and diarrhea.3,11 Hepatitis, thrombocytopenia, and encephalitis occur less commonly. Thrombocytopenia-associated purpura may be severe. Pneumonia is the most common fatal complication of measles in children and the most common complication overall in adults. The disease severity is worse in immunocompromised and malnourished individuals,
often resulting in the development of Hecht giant cell pneumonia.
Differential Diagnosis of Measles
Most Likely
- · Drug hypersensitivity reaction
- · Rubella
Consider
- · Rocky Mountain spotted fever (atypical cases)
- · Henoch-Schönlein purpura (atypical cases)
- · Other viral infection (parvovirus, enterovirus, adenovirus, human herpesvirus-6, Epstein-Barr virus)
Always Rule Out
- · Kawasaki disease
- · Graft-versus-host disease (recent bone marrow transplant)
Prognosis and Clinical Course
Clinical diagnosis of measles is typically made with onset of the characteristic rash as the prodromal symptoms can mimic influenza-like illnesses. Uncomplicated measles is self-limited, lasting 10 to 12 days. Malnutrition, immunosuppression, poor health, and inadequate supportive care can worsen the prognosis in any patient. In developing nations, measles is a major cause of infant mortality.
Treatment
Treatment for measles in the majority of cases is supportive. Patients with secondary bacterial infections need to be treated with appropriate antibiotics. Ribavirin may be considered, as it has been shown to inhibit measles virus in tissue culture and reduce the severity and duration of measles in some cases.2,3,18 In trials with patients with subacute sclerosing panencephalitis, however, no benefit was noted with the use of ribavirin.
Malnutrition and vitamin A deficiency can depress cell-mediated immunity in children, increasing the risk and severity of childhood infections. Measles virus infection decreases serum levels of vitamin A and can lead to higher risk of mortality from disease. Vitamin A supplementation is recommended for all children with measles who live in communities where vitamin A deficiency is known or where measles fatality rate is 1 percent.3,19 In the United States, supplementation is considered for children 6 months to 2 years who are hospitalized with measles and its complications or for children more than 6 months of age who are at risk for vitamin A deficiency (immunodeficiency, severe malnutrition).3 More recent studies of vitamin A have led to some controversy regarding its use.20
All individuals at risk (children less than 1 year of age, pregnant women, unimmunized, immunocompromised, exposed to measles virus) should receive immunoglobulin prophylaxis within 6 days of exposure.3 If given within 72 hours of exposure, the individual will not be infected with the virus.2 Healthy individuals should receive 0.25 mL/kg of intramuscular immunoglobulin, and immunocompromised patients require 0.5 mL/kg.3 Exposed patients (excluding pregnant women and those with impaired immune systems) should also be given the measles vaccine 5 months later to confer lasting protection .
Treatments for Measles
- o Supportive care
- o Treat secondary infections
- o Vitamin Aa
- o Immune globulin, IMa
- o Measles vaccine
- o Ribavirina
Prevention (Immunizations)
The incidence of measles has decreased worldwide as a direct result of immunization. A single dose of the live attenuated measles vaccine produces detectable levels of antibody in 95 percent of individuals, conferring lifelong immunity.
Common potential side effects of measles vaccine include fever and transient morbilliform rash that resolve without treatment. Less common adverse reactions include thrombocytopenia and transient neurologic reactions.
Measles vaccine administration is contraindicated in individuals who have a moderate to severe illness as well as those allergic to eggs or neomycin. It is also contraindicated in pregnant women and those with impaired immune systems [cancer, non-human immunodeficiency virus (HIV) immune deficiency disease, immunosuppressive therapy]. Patients off chemotherapy or immunosuppressive medications for 3 months can receive the measles vaccine.
There have been many unconfirmed, unsubstantiated but widely publicized reports suggesting a potential link between measles-mumps-rubella (MMR) vaccine and the development of autism and possibly inflammatory bowel disease. Current scientific evidence does not support a causal link between MMR vaccine and autism or inflammatory bowel disease