Protein Energy Malnutrition
The World Health Organization (WHO) defines malnutrition as "the cellular imbalance between the supply of nutrients and energy and the body's demand for them to ensure growth, maintenance, and specific functions." The term protein-energy malnutrition (PEM) applies to a group of related disorders that include marasmus, kwashiorkor, and intermediate states of marasmus-kwashiorkor. The term marasmus is derived from the Greek word marasmos, which means withering or wasting. Marasmus involves inadequate intake of protein and calories and is characterized by emaciation. The term kwashiorkor is taken from the Ga language of Ghana and means "the sickness of the weaning." Williams first used the term in 1933, and it refers to an inadequate protein intake with reasonable caloric (energy) intake. Edema is characteristic of kwashiorkor but is absent in marasmus.
Studies suggest that marasmus represents an adaptive response to starvation, whereas kwashiorkor represents a maladaptive response to starvation. Children may present with a mixed picture of marasmus and kwashiorkor, and children may present with milder forms of malnutrition. For this reason, Jelliffe suggested the term protein-calorie (energy) malnutrition to include both entities.
Although protein-energy malnutrition affects virtually every organ system, this article primarily focuses on its cutaneous manifestations. Patients with protein-energy malnutrition may also have deficiencies of vitamins, essential fatty acids, and trace elements, all of which may contribute to their dermatosis.
In general, marasmus is an insufficient energy intake to match the body's requirements. As a result, the body draws on its own stores, resulting in emaciation. In kwashiorkor, adequate carbohydrate consumption and decreased protein intake lead to decreased synthesis of visceral proteins. The resulting hypoalbuminemia contributes to extravascular fluid accumulation. Impaired synthesis of B-lipoprotein produces a fatty liver.
Protein-energy malnutrition also involves an inadequate intake of many essential nutrients. Low serum levels of zinc have been implicated as the cause of skin ulceration in many patients. In a 1979 study of 42 children with marasmus, investigators found that only those children with low serum levels of zinc developed skin ulceration. Serum levels of zinc correlated closely with the presence of edema, stunting of growth, and severe wasting. The classic "mosaic skin" and "flaky paint" dermatosis of kwashiorkor bears considerable resemblance to the skin changes of acrodermatitis enteropathica, the dermatosis of zinc deficiency.
In 2007, Lin et al2 stated that "a prospective assessment of food and nutrient intake in a population of Malawian children at risk for kwashiorkor" found "no association between the development of kwashiorkor and the consumption of any food or nutrient."
Protein-energy malnutrition is the most common form of nutritional deficiency among patients who are hospitalized in the United States. As many as half of all patients admitted to the hospital have malnutrition to some degree. In a recent survey in a large children's hospital, the prevalence of acute and chronic protein-energy malnutrition was more than one half.
In a survey focusing on low-income areas of the United States, 22-35% of children aged 2-6 years were below the 15th percentile for weight. Another survey showed that 11% of children in low-income areas had height-for-age measurements below the 5th percentile. Poor growth is seen in 10% of children in rural populations.
In hospitalized elderly persons, up to 55% are undernourished. Up to 85% of institutionalized elderly persons are undernourished. Studies have shown that up to 50% have vitamin and mineral intake that is less than the recommended dietary allowance and up to 30% of elderly persons have below-normal levels of vitamins and minerals.
In 2000, the WHO estimated that malnourished children numbered 181.9 million (32%) in developing countries. In addition, an estimated 149.6 million children younger than 5 years are malnourished when measured in terms of weight for age. In south central Asia and eastern Africa, about half the children have growth retardation due to protein-energy malnutrition. This figure is 5 times the prevalence in the western world.
- Approximately 50% of the 10 million deaths each year in developing countries occur because of malnutrition in children younger than 5 years.
- In kwashiorkor, mortality tends to decrease as the age of onset increases.
Dermatologic findings appear more significant and occur more frequently among darker-skinned peoples. This finding is likely explained by the greater prevalence and the increased severity of protein-energy malnutrition in developing countries and not to a difference in racial susceptibility.
Marasmus most commonly occurs in children younger than 5 years. This period is characterized by increased energy requirements and increased susceptibility to viral and bacterial infections. Weaning (the deprivation of breast milk and the commencement of nourishment with other food) occurs during this high-risk period. Weaning is often complicated by geography, economy, hygiene, public health, culture, and dietetics. It can be ineffective when the foods introduced provide inadequate nutrients, when the food and water are contaminated, when the access to health care is inadequate, and/or when the patient cannot access or purchase proper nourishment.
In some studies, the protein-energy malnutrition prevalence among elderly persons is estimated to be as high as 4% for those living in the community, 50% for those hospitalized in acute care units or geriatric rehabilitation units, and 30-40% for those in long-term care facilities. Protein-energy malnutrition has also been found to be a primary factor of poor prognosis in elderly persons.
Low intake of calories or an inability to absorb calories is the key factor in the development of kwashiorkor.
- In children, the findings of poor weight gain or weight loss; slowing of linear growth; and behavioral changes, such as irritability, apathy, decreased social responsiveness, anxiety, and attention deficit may indicate protein-energy malnutrition. In particular, the child is apathetic when undisturbed but irritable when picked up.
- Kwashiorkor characteristically affects children who are being weaned. Signs include diarrhea and psychomotor changes.
- Adults generally lose weight, although, in some cases, edema can mask weight loss. Patients may describe listlessness, easy fatigue, and a sensation of coldness. Global impairment of system function is present.
- Patients with protein-energy malnutrition can also present with nonhealing wounds. This may signify a catabolic process that requires nutritional intervention.
- Lewandowski et al4 reported kwashiorkor and an acrodermatitis enteropathica–like eruption after a distal gastric bypass surgical procedure.
- Kwashiorkor was reported in an infant presenting with diarrhea and dermatitis, due to infantile Crohn disease.5 The diarrhea and dermatitis improved in 2 weeks with treatment.
- A 3-year-old child with coexisting celiac and Hartnup disease that resulted in kwashiorkor, anemia, hepatitis, hypoalbuminia, angular cheilitis, glossitis, conjunctivitis and diffuse alopecia, erythematous skin, desquamation, erosions, and diffuse hyperpigmentation was reported by Sander et al in 2009.6 With the proper nutritional supplementation, these findings resolved.
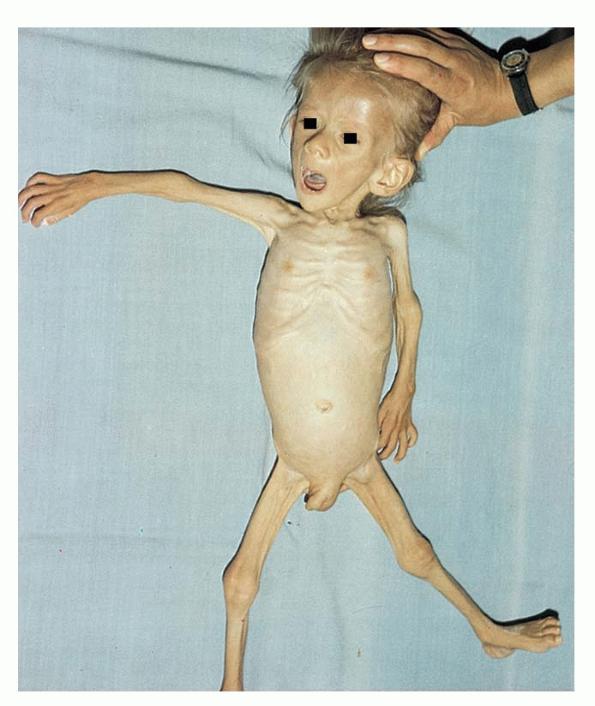
In marasmus, the child appears emaciated with marked loss of subcutaneous fat and muscle wasting. The skin is xerotic, wrinkled, and loose. Monkey facies secondary to a loss of buccal fat pads is characteristic of this disorder. Marasmus may have no clinical dermatosis. However, inconsistent cutaneous findings include fine, brittle hair; alopecia; impaired growth; and fissuring of the nails. In protein-energy malnutrition, more hairs are in the telogen (resting) phase than in the anagen (active) phase, a reverse of normal. Occasionally, as in anorexia nervosa, marked growth of lanugo hair is noted.
Kwashiorkor typically presents with a failure to thrive, edema, moon facies, a swollen abdomen (potbelly), and a fatty liver. When present, skin changes are characteristic and progress over a few days. The skin becomes dark, dry, and then splits open when stretched, revealing pale areas between the cracks (ie, crazy pavement dermatosis, enamel paint skin). This feature is seen especially over pressure areas. In contrast to pellagra, these changes seldom occur on sun-exposed skin.
Depigmentation of hair causes it to be reddish yellow to white. Curly hair becomes straightened. If periods of poor nutrition are interspersed with good nutrition, alternating bands of pale and dark hair, respectively, called the flag sign, may occur. Also, hairs become dry, lusterless, sparse, and brittle; they can be pulled out easily. Temporal recession and hair loss from the back of the head occur, likely secondary to pressure when the child lies down. In some cases, loss of hair can be extreme. Hair can also become softer and finer and appear unruly. The eyelashes can undergo the same change, having a so-called broomstick appearance.
Nail plates are thin and soft and may be fissured or ridged. Atrophy of the papillae on the tongue, angular stomatitis, xerophthalmia, and cheilosis can occur.
Inflammatory bowel diseases, such as Crohn disease and ulcerative colitis, may also produce skin manifestations secondary to malnutrition.
In elderly persons, an indicative sign of malnutrition is delayed healing and an increased presence of decubitus ulcers of stage III or higher.
Vitamin C deficiency commonly manifests in elderly persons as perifollicular hemorrhages, petechiae, gingival bleeding, and splinter hemorrhages, in addition to hemarthroses and subperiosteal hemorrhages. Anemia may result, and wound healing may be impaired. Niacin deficiency clinically manifests as pellagra (ie, dermatitis, dementia, diarrhea) in advanced cases. The dermatitis manifests in sun-exposed areas, including the back, neck (Casal necklace), face, and dorsum of the hands (gauntlet of pellagra) initially as painful erythema and itching. Subsequently, vesicles and bullae may develop and erupt, creating crusted, scaly lesions. Finally, the skin becomes rough and covered by dark scales and crusts. Striking demarcation of affected areas from normal skin is noted.
Protein-energy malnutrition is also associated with an increased likelihood of calciphylaxis, a small vessel vasculopathy involving mural calcification with intimal proliferation, fibrosis, and thrombosis. As a result, ischemia and necrosis of skin occurs. Other tissues affected include subcutaneous fat, visceral organs, and skeletal muscle.
Causes
Worldwide, the most common cause of malnutrition is inadequate food intake. Preschool-aged children in developing countries are often at risk for malnutrition because of their dependence on others for food, increased protein and energy requirements, immature immune systems causing a greater susceptibility to infection, and exposure to nonhygienic conditions.
Another significant factor is ineffective weaning secondary to ignorance, poor hygiene, economic factors, and cultural factors. The prognosis is worse when protein-energy malnutrition occurs with HIV infection. Gastrointestinal infections can and often do precipitate clinical protein-energy malnutrition because of associated diarrhea, anorexia, vomiting, increased metabolic needs, and decreased intestinal absorption. Parasitic infections play a major role in many parts of the world.
In developed countries, inadequate food intake is a less common cause of malnutrition; protein-energy malnutrition is more often caused by decreased absorption or abnormal metabolism. Thus, in developed countries, diseases, such as cystic fibrosis, chronic renal failure, childhood malignancies, congenital heart disease, and neuromuscular diseases, contribute to malnutrition. Fad diets, inappropriate management of food allergies, and psychiatric diseases, such as anorexia nervosa, can also lead to severe protein-energy malnutrition.
Populations in both acute-care and long-term facilities are at risk for clinically significant involuntary weight loss (IWL) that can result in protein-energy malnutrition. IWL is defined as a loss of 4.5 kg or greater than 5% of the usual body weight over a period of 6-12 months. Protein-energy malnutrition occurs when weight loss of greater than 10% of normal body weight occurs.
Elderly persons often develop malnutrition, common causes of which include decreased appetite, dependency on help for eating, impaired cognition and/or communication, poor positioning, frequent acute illnesses with gastrointestinal losses, medications that decrease appetite or increase nutrient losses, polypharmacy, decreased thirst response, decreased ability to concentrate urine, intentional fluid restriction due to fear of incontinence or choking if dysphagic, psychosocial factors such as isolation and depression, monotony of diet, higher nutrient density requirements, and other demands of age, illness, and disease on the body.
Elderly patients are often at risk for protein-energy malnutrition because of inadequate nutrition, which has been determined to be a common comorbid factor for increased morbidity and mortality in elderly burn victims.
Patients with liver cirrhosis are also at risk for protein-energy malnutrition, which is a risk factor that portends a poor prognosis for survival. This risk correlates with the degree of liver injury and the etiology of liver injury, with the risk of protein-energy malnutrition being more severe in persons with alcoholic cirrhosis than in those with nonalcoholic cirrhosis.
Patients on long-term hemodialysis also may develop protein-energy malnutrition; this is associated with increased morbidity and mortality.
Patients with squamous cell carcinoma of the esophagus are at risk for protein-energy malnutrition.