| Keratosis Pilaris =التقران الجرابي |
|
|
KERATOSIS PILARIS
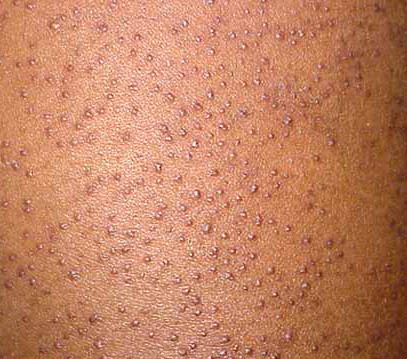
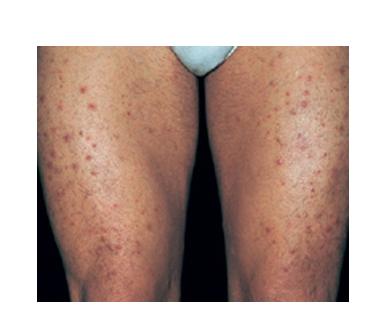
Isolated typical KP is a common condition of keratotic follicular plugging with varying degrees of surrounding erythema. Sometimes, the erythema is so striking that it is the main complaint. The clinical expression of KP varies from very subtle to very conspicuous, which, along with possible racial differences, may explain the great range of reported prevalences, from 1 percent to 42 percent. It involves, particularly, the extensor aspects of the upper arms and thighs as well as the face but may rarely be more extensive, extending to the distal limbs and even the trunk. There seem to be two patterns. The more common one is commencement in early childhood, in most cases before 2 years of age, with face and arms mainly affected and gradual improvement in most cases by later childhood or adolescence. In the other pattern, the onset is in teenage years, and the extensor arms and legs are predominantly involved. It usually improves by the mid-20s. In both patterns, however, the condition may be persistent into later adult life. The histopathologic pattern in skin biopsy specimens is nonspecific, simply showing the follicular orifice distended by a keratin plug. Treatment is usually with various keratolytics, from simple urea, lactic acid, or salicylic acid preparations to topical retinoids and tazarotene. These preparations may aggravate associated erythema, limiting their value.
KERATOSIS PILARIS AT A GLANCE · Common condition of keratotic follicular plugging with variable erythema. · Mainly involves cheeks and extensor arms and thighs. · Two main patterns—early childhood onset and adolescent onset. · Usually improves gradually over years. · Non-specific histology of follicular orifice distended by keratin plug. · Variable response to keratolytics. · Erythromelanosis follicularis faciei et colli is a variant with marked erythema and hyperpigmentation.
|