















































Actinic keratoses
Actinic keratosis (AK) is a UV light–induced lesion of the skin that may progress to invasive squamous cell carcinoma.1,2,3 It is by far the most common lesion with malignant potential to arise on the skin. Actinic keratosis is seen in fair-skinned persons on skin areas that have had long-term sun exposure.4 In Australia, the country with the highest skin cancer rate in the world, the prevalence of actinic keratosis among adults older than 40 years has been reported to range from 40-60%.5
The premalignant nature of actinic keratosis was recognized almost 100 years ago, and the name literally means thickened scaly growth (keratosis) caused by sunlight (actinic). In the United States, actinic keratosis represents the second most frequent reason for patients to visit a dermatologist.6
An actinic keratosis may follow 1 of 3 paths; it may regress, it may persist unchanged, or it may progress to invasive squamous cell carcinoma. The actual percentage that progress to invasive squamous cell carcinoma remains unknown, and estimates have varied from as low as 0.1% to as high as 10%.1,7 Early data suggest that actinic keratoses may also progress to basal cell carcinoma, a paradigm originally not considered in the actinic keratosis risk profile.8
In 2009, Criscione and colleagues conducted a study examining the progression of actinic keratoses to squamous cell carcinoma and basal cell carcinoma. The study examined 7784 actinic keratoses in a high-risk population and found that nearly 65% of primary squamous cell carcinomas and 36% of primary basal cell carcinomas arise from clinically diagnosed actinic keratoses. Furthermore, risk of progression of actinic keratosis to squamous cell carcinoma was 0.60% at 1 year and 2.57% at 4 years, which is 6-8 times more frequent than has been reported in some prior studies. The risk of progression of actinic keratosis to basal cell carcinoma was 0.48% at 1 year and 1.97 at 4 years, although it is acknowledged that it is possible that many of these lesions may have been previously mistaken for actinic keratoses.9
Although it is impossible to predict which individual lesion will follow which course, as most patients have many lesions, accessing risk becomes more significant and aids in tailoring treatments. Overall, actinic keratoses can be safely and effectively eradicated, and, therefore, therapy is warranted.
Pathophysiology
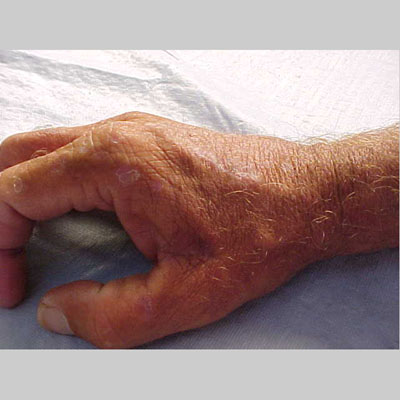
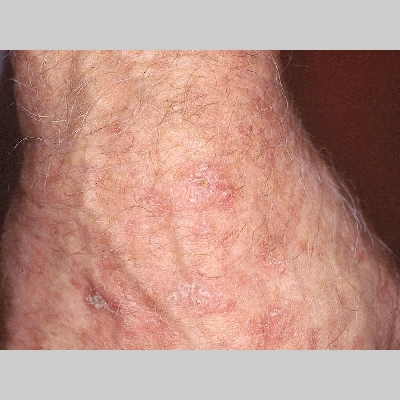
Actinic keratoses arise on fair-skinned people in areas of long-term sun exposure, such as the face, ears, bald scalp, forearms, and backs of the hands.4 However, they may occur on any area that is repeatedly exposed to the sun, such as the back, the chest, and the legs. Long-term UV light exposure is implicated as the cause from both epidemiologic observations and molecular analysis of tumor cells.2,4 Actinic keratosis frequency correlates with cumulative UV exposure.4 Therefore, the frequency of actinic keratosis increases with each decade of life, is greater in residents of sunny countries closer to the equator, and is greater in persons with outdoor occupations.4,10 DNA analysis of the cells within actinic keratoses shows characteristic UV-induced mutations in key genes, including TP53 and deletion of the gene coding for p16 tumor suppressor protein.2,11,12
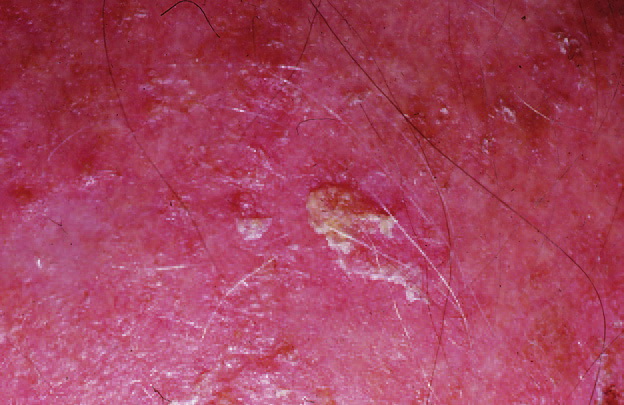
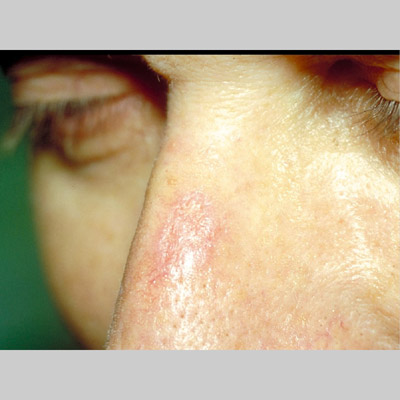
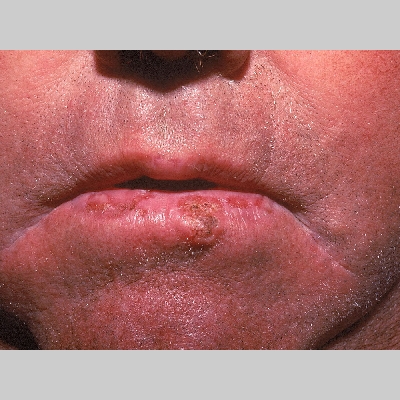
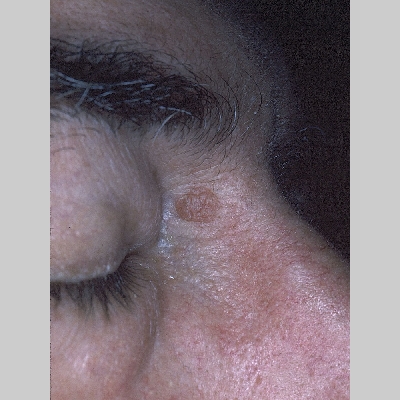
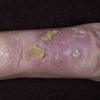
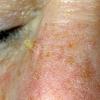
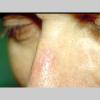
Clinically, actinic keratoses range from barely perceptible rough spots of skin to elevated, hyperkeratotic plaques several centimeters in diameter.13 Most often, they appear as multiple discrete, flat or elevated, keratotic lesions. Lesions typically have an erythematous base covered by scale (hyperkeratosis).13 They are usually 3-10 mm in diameter and gradually enlarge into broader, more elevated lesions.
Over time, actinic keratoses may develop into invasive squamous cell carcinoma; according to one study of almost 7000 patients, among the small percentage of actinic keratoses that progress into squamous cell carcinoma, the length of time for this transformation to occur was approximately 2 years.14 Development of actinic keratoses may occur as early as the third or fourth decade of life in patients who live in areas of high solar radiation, are fair-skinned, and do not use sunscreen for photoprotection.4 Usually, patients demonstrate a background of solar-damaged skin with telangiectasias, elastosis, and pigmented lentigines.15
In both histologic and molecular parameters, actinic keratoses share features with squamous cell carcinoma.16 Actinic keratosis is an epidermal lesion characterized by aggregates of atypical, pleomorphic keratinocytes at the basal layer that may extend upwards to involve the granular and cornified layers.16 The epidermis itself shows an abnormal architecture, with acanthosis, parakeratosis, and dyskeratosis. Cellular atypia is present, and the keratinocytes vary in size and shape; mitotic figures are present.16 This presentation may resemble Bowen disease or carcinoma in situ, and the distinction between the 2 is a matter of degree (extent of the lesion) rather than differences in individual cells.16
Often, marked hyperkeratosis and areas of parakeratosis with loss of the granular layer are present. A dense inflammatory infiltrate is usually present. The case has been made that actinic keratosis is the earliest manifestation of squamous cell carcinoma and should be regarded as such rather than as a precancerous lesion.16,17 Others have argued that calling actinic keratosis a carcinoma unduly alarms patients. Cockerell has proposed renaming the lesion keratinocytic intraepidermal neoplasia, using a nomenclature analogous to cervical and vulvar intraepithelial neoplasia.16
Mortality/Morbidity
Lesions begin as barely perceivable rough spots of skin, better felt than seen.15,20 Early lesions feel like sandpaper; later lesions become erythematous, scaly plaques that may enlarge to several centimeters.4,15 Lesions may remain unchanged for years, may spontaneously regress, or may progress to invasive squamous cell carcinoma.7 Most actinic keratoses do not progress to invasive squamous cell carcinoma; however, most invasive squamous cell carcinomas have evidence of a preexisting actinic keratosis.4,7 Invasive squamous cell carcinoma may produce significant morbidity by direct extension into facial structures. In less than 10% of cases, invasive squamous cell carcinoma may metastasize, with a low 5-year survival rate.
History
Actinic keratoses are seen almost exclusively in whites, especially those with skin phototypes I and II.10 The incidence increases with each decade of life, and men have a slightly increased frequency of actinic keratosis.5,10 Actinic keratosis is correlated with long-term UV exposure, such as occurs in persons with outdoor occupations.10
Patient who are immunosuppressed following organ transplantation are at markedly increased risk of developing actinic keratoses.24 The lesions still arise in areas of long-term exposure,14,25,26 and they are thought to be actinically induced.
Physical
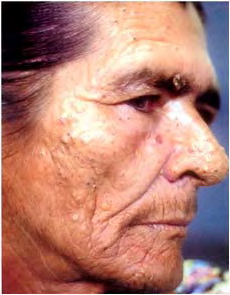
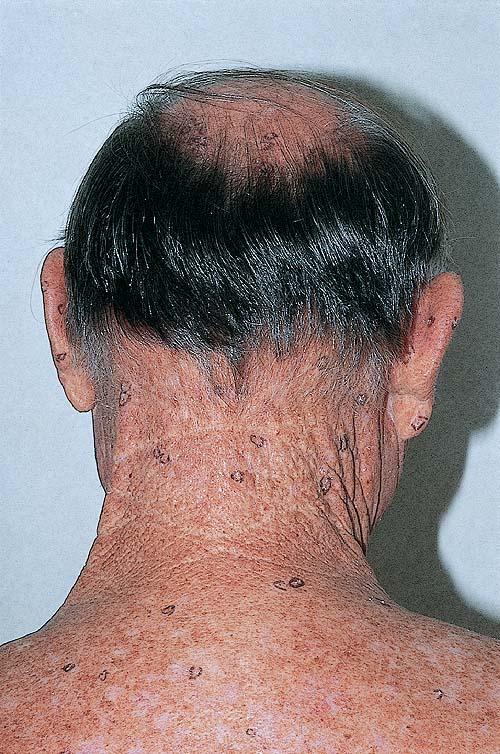
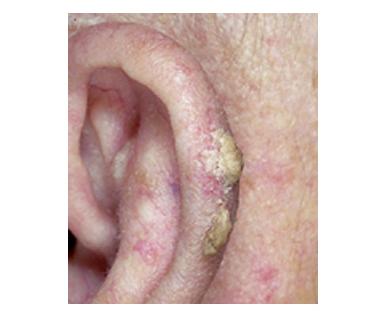
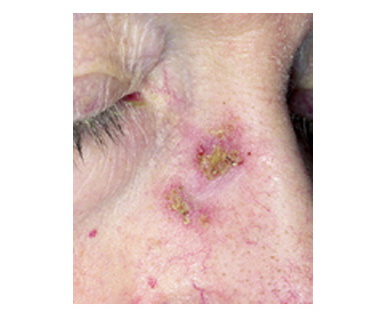
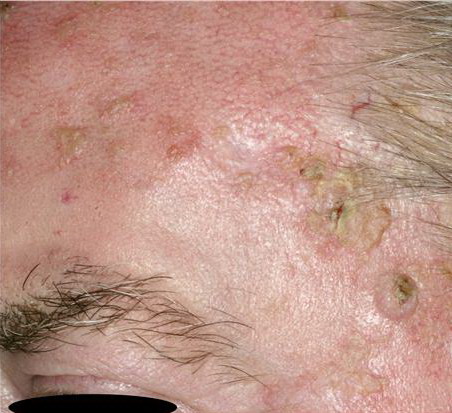
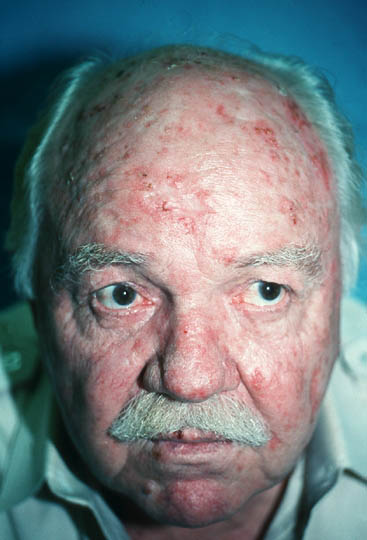
The typical patient with actinic keratoses is an elderly, fair-skinned, sun-sensitive person.10 The lesions arise in areas of long-term sun exposure, including the face, ears, bald scalp in men, and the dorsal forearms and hands.4,25 Actinic keratoses begin as small rough spots that are easier felt than seen, often described as being similar to rubbing sandpaper.15 With time, the lesions enlarge, usually becoming red and scaly; most are only 3-10 mm, but they may enlarge to several centimeters.15,27,28 Note the images below.
Patients may develop multiple lesions within a single anatomic area, to the extent that the lesions collide and produce confluent actinic keratosis over a relatively large area. Variants may be brown (pigmented actinic keratosis), atrophic, bowenoid, lichen planus–like, or have exaggerated hyperkeratosis, producing a hornlike projection above the skin surface known as a cutaneous horn.29
Causes
Actinic keratoses are induced by UV light. Both epidemiologic observations and molecular biologic characteristics of the tumor cells suggest UV light is sufficient by itself to induce actinic keratosis.2,12 Sensitivity to UV light is inherited; actinic keratoses occur more frequently in fair, redheaded, or blonde patients who burn frequently and tan poorly.4 Increased sun exposure and higher-intensity exposure increase the chance of actinic keratosis development. Immunosuppression following organ transplantation dramatically increases the risk of developing actinic keratoses24 ; however, actinic keratoses do not occur without sun exposure.
Additional studies have shown an association between cutaneous human papillomavirus and actinic keratosis.30,31,32 The role of human papillomavirus in skin tumorigenesis was discovered the 1950s, and the group of known human papillomavirus types associated with skin tumorigenesis has been classified as beta-papillomavirus .31 Beta-papillomavirus DNA has been identified in healthy skin and in squamous cell carcinoma, basal cell carcinoma, and actinic keratosis. A 2007 study suggests that only a small association exists between beta-papillomavirus and actinic keratosis; however, when evaluated in combination with other risk factors including age, sun damage, and skin color, the risk for actinic keratosis increased as much as 13-fold.31 The exact mechanism by which this family of viruses contributes to tumor growth remains unknown.
Histologic Findings
Actinic keratosis is characterized by dysplasia and architectural disorder of the epidermis.15 Keratinocytes of the basal layer are abnormal and are variable in size and shape; cellular polarity is altered, and nuclear atypia is seen.15 These alterations may extend upward to the granular layer, which may be thinned. Overall, the epidermis exhibits hyperkeratosis and parakeratosis, and irregular acanthosis may be present.15 In general, hair follicles, sebaceous glands, and apocrine and eccrine ducts are not involved
Medical Care
Actinic keratoses may remain unchanged, spontaneously resolve, or progress to invasive squamous cell carcinoma.15 The fate of any one actinic keratosis is impossible to predict. Although the risk of progression of any one actinic keratosis to invasive squamous cell carcinoma is small (at most approximately 10%),1 a patient may have many lesions, and thus the risk of progression becomes significant. Additionally, actinic keratoses can be clinically indistinguishable from more serious cutaneous malignancies, including squamous cell carcinoma and lentigo maligna.35,36 Therapy is generally well tolerated and simple; therefore, treatment of all actinic keratoses is warranted.
The appropriate treatment is generally chosen based on the number of lesions present and the efficacy of the treatment.37 Additional variables to consider include persistence of the lesion(s), age of the patient, history of skin cancer, and tolerability of the treatment modality.1 Treatment consists of 2 broad categories: surgical destruction of the lesion and medical therapy. Medical management begins with educating the patient to limit sun exposure. Patients should be cautioned to avoid sun exposure from 10:00 am to 3:00 pm as much as possible. They also must wear adequate sunscreens and protective clothing daily.38
Medical therapy has the advantage of being able to treat large areas with many lesions. The disadvantages of medical therapies include lengthy courses of treatment with irritation and discomfort. The US Food and Drug Administration (FDA) has approved 4 medications for the treatment of actinic keratoses. These are topical 5-fluorouracil (5-FU), 5% and 3.75% imiquimod cream, topical diclofenac gel, and PDT with topical delta-aminolevulinic acid.39,40,41
5-Fluorouracil
The most experience in topical therapy for actinic keratoses is with 5-FU, known to inhibit thymidylate synthetase and cause cell death in actively proliferating cells.42 Several formulations are available, including a 5% cream or solution, a 2% solution, a 1% cream or solution, and, most recently, a micronized 0.5% cream.39 Although not well studied, efficacy among the various formulations does not seem to differ significantly.43,44
The most popular formulation is the 5% cream, which is applied twice daily for 1 month. During the treatment phase, the lesions become increasingly erythematous and cause discomfort; small subclinical lesions become visible. This treatment can be temporarily disfiguring, with erythematous ulcerations and crust formation. However, if the patient completes the treatment, the lesions usually heal within 2 weeks of stopping treatment, the complexion is smooth, and the actinic keratoses are improved.
The 0.5% micronized cream was developed to increase tolerability because inflammation and discomfort can be a limiting factor in the use of topical 5-FU. The 0.5% micronized cream is applied once daily for 1 month.
Usage of the 0.5% micronized cream 1 week prior to cryosurgery has also been shown to produce complete lesion clearance in a higher number of patients compared with cryosurgery alone (32.4% and 15%, respectively).
Imiquimod
Imiquimod is a topical medication that up-regulates a variety of cytokines, which, in turn, invoke a nonspecific immune response (interferons, natural killer cells) and a specific immune response (T cells). It is applied 2-3 times a week for up to 4 months, although generally 1 month is sufficient.46 Reaction to the drug is idiosyncratic, with some patients barely reacting and others developing marked inflammation. Subclinical lesions previously not appreciated may become inflamed during therapy. In patients with a brisk inflammatory response, dosing is reduced to twice or even once a week, with preservation of therapeutic efficacy but increased tolerability.
Two new formulations of imiquimod (2.5% and 3.75%) were studied and found to be efficacious in clearing actinic keratoses (25% and 34% clearance, respectively), with a more intuitive daily dosing schedule. Although not as efficacious as 5% imiquimod, the new formulations cause less irritation, promoting better compliance.47 Experimental evidence suggests patients may develop T-cell memory after treatment with this drug and thus may be less likely to develop new actinic keratoses in the future. Imiquimod 5% cream has also been shown to be safe and effective in transplantation patients.48,49
Topical diclofenac sodium 3% gel
Topical diclofenac sodium 3% gel is a nonsteroidal anti-inflammatory drug approved by the FDA for the treatment of actinic keratosis. Its mechanism of action against actinic keratoses is unknown. It is effective therapy when applied twice a day for 3 months. A shorter course of therapy is dramatically less effective. Its chief advantage is that it produces little-to-no inflammation and thus is very well tolerated. Diclofenac therapy after cryosurgery has also been shown to produce complete lesion clearance in a higher number of patients compared with cryosurgery alone (64% vs 32%, respectively).50
Photodynamic therapy
PDT uses a light-sensitizing compound that preferentially accumulates in actinic keratosis cells, where it can be activated by the appropriate wavelength of light. Delta-aminolevulinic acid is a component of the heme biosynthetic pathway that accumulates preferentially in dysplastic cells. Once inside these cells, it is enzymatically converted to protoporphyrin IX, a potent photosensitizer. With exposure to light of an appropriate wavelength, oxygen free radicals are generated and cell death results.51
Patients experience pain, similar in scope to the pain resulting from topical 5-FU, in the areas treated. The treated lesions may become erythematous and crusted. One treatment with PDT appears to be as effective as topical 5-FU therapy.52
Immunosuppressed patients may also benefit from PDT in the prevention of nonmelanoma skin cancers.53
When used with light sources that have a cosmetic benefit by themselves, such as the pulsed dye laser or intense pulsed light devices, a cosmetic benefit may be seen from the use of topical PDT beyond that of actinic keratosis eradication. Compared with other destructive therapeutic options such as cryotherapy, PDT may offer better cosmetic results and higher patient preference.53,54
An unknown parameter in the use of topical PDT is the optimal incubation time following application of the topical aminolevulinic acid before light exposure. A second unknown parameter is the optimal light source to use for this treatment. Ongoing studies are addressing these issues.53,55
Surgical Care
The goal of surgical therapy is complete eradication of the actinic keratoses, usually by physical destruction, with limited-to-no damage to surrounding healthy tissue. When the diagnosis is unclear and an invasive tumor is possible, biopsy is indicated. However, biopsy generally leaves a scar.
Cryosurgery refers to use of a cryogen to lower the temperature of the skin and produce cell death. The most common cryogen used is liquid nitrogen, with a temperature of -195.8°C. Keratinocytes die when exposed to approximately -40 to -50°C. Other structures in the skin, such as collagen, blood vessels, and nerves, are more resistant to the lethal effects of cold than keratinocytes. Melanocytes are more sensitive than keratinocytes; thus, cryosurgery often leaves white spots. This technique has not been studied in a scientific fashion until 2004, when it was demonstrated to produce an overall clearance rate of 67-88%.54,56
Lesions suggestive of invasive cancer may be treated with curettage, shave excision, or conventional excision, all of which provide a sample for histologic evaluation. These treatments require local anesthesia, produce a wound that requires time to heal, and are likely to scar.
Cosmetic resurfacing procedures, in which the entire epidermis is removed, sometimes with some portion of the dermis, are effective for actinic keratosis eradication. Cosmetic resurfacing procedures include medium and deep chemical peels, dermabrasion, and ablative laser resurfacing.57,58,59 All of these are cosmetic procedures unlikely to be covered by insurance, all carry the risk of scarring and infection, and all require experience and expertise on the part of the dermatologic surgeon. They are highly unlikely to be performed solely for actinic keratosis therapy